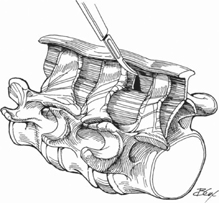
76 Kern Singh and Frank M. Phillips Biomechanical studies have suggested that the restriction of segmental motion resulting from spinal fusion causes abnormal kinematics at adjacent mobile segments, potentially leading to instability and accelerated degeneration. In an attempt to eliminate problems innate to fusion surgery, the concept of dynamically stabilizing a diseased lumbar motion segment has been proposed. Theoretically, an interspinous process device should assist in the functioning of the diseased motion segment by providing stability while allowing motion and by load-sharing the forces transmitted through the posterior spinal elements. The device for intervertebral assisted motion (DIAM) and the Wallis system are interspinous process “bumpers” designed to provide facet distraction, decrease intradiskal pressure, and reduce abnormal segmental motion and alignment. Indications for using interspinous prostheses remain poorly defined and largely reflect individual surgeon biases. The DIAM and Wallis devices have been used in the following situations: Isthmic spondylolysis, unstable spondylolisthesis (higher than grade I), neoplasia, fracture, and idiopathic scoliosis. Relative contraindications include osteoporotic bone and stable degenerative spondylolisthesis (grade I). Preoperative imaging is essential to determine the etiologic and anatomic sites of neural compression. Plain radiographs, in addition to magnetic resonance imaging (MRI) or myelography and postmyelogram computed tomography (CT) imaging, are essential for identifying sites of neural compression and for identifying degenerative spinal pathologies. Traditional fusion procedures disrupt the normal segmental musculature and the inherent dynamic stabilization of the spine, likely degrading the surgical outcome. As such, the DIAM conforms to the interspinous anatomy and allows placement with minimal disturbance of the segmental muscles through a simple midline approach with preservation of the segmental anatomy. Patient is positioned in the standard prone position. These devices may be placed under local or general anesthesia. The most frequently involved anatomic level is L4-L5. The surgical approach is performed using a standard midline incision or a slightly lateral incision (10 mm lateral to the midline). A counterincision is necessary for insertion, preparation, and seating of the device. Care must be taken to maintain continuity of the supraspinous ligament by preserving a band at least 10 mm wide and as thick as possible. A window is created in the interspinous space using a scalpel that is ideally curved upward; the window is then enlarged with a curved Kerrison rongeur, taking care to preserve cortical bone (Fig. 76.1). At this stage, the interlaminar distractor can be inserted as far anteriorly as possible at the junction between the base of the spinous process and the laminae (Fig. 76.2). The appropriate trial (sizes available in 2-mm increments, from 8 to 14 mm) is positioned between the grooves of the distractor to determine the implant size (Fig. 76.3). Proper fit of the interspinous prosthesis should be based on re-tensioning of the supraspinous ligament and realignment of the facets and articular capsule (Fig. 76.4). Parallel alignment of the end plates can also be used as a reference for re-tensioning of the posterior longitudinal ligament. Pressing the trigger of the inserter both activates the claw and pulls back the arms of the inserter, allowing the wings to unfold, bringing them into contact with the spinous processes. The impactor is placed on top of the implant and the prosthesis is pushed down with gentle taps of the mallet. The posterior interspinous stabilizer is packaged with two independent ligaments that attach respectively to each adjacent spinous process (Fig. 76.5). The rivet is brought down to the loop, tensioned, and secured with the crimper. The rest of the ligament is cut off and removed.
Posterior Interspinous Implant Placement
Description
Key Principles
Expectations
Indications
Contraindications
Special Considerations
Special Instructions, Position, and Anesthesia
Tips, Pearls, and Lessons Learned
Related posts:
 Anterior Thoracic and Thoracolumbar Plating Techniques
Anterior Thoracic and Thoracolumbar Plating Techniques
 Anterior Cervical Corpectomy
Anterior Cervical Corpectomy
 Minimally Invasive Posterior Surgical Approaches to the Lumbar Spine Through Tubular Retractors
Minimally Invasive Posterior Surgical Approaches to the Lumbar Spine Through Tubular Retractors
 Open Lumbar Microscopic Diskectomy
Open Lumbar Microscopic Diskectomy
 Spondylolysis Repair (Pars Interarticularis Repair)
Spondylolysis Repair (Pars Interarticularis Repair)
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


