TABLE 43.1 Approximate Frequency of Clinical Features of Posterior Reversible Encephalopathy Syndrome | ||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
regions between the major vascular territories. These include progressive multifocal leukoencephalopathy, encephalitis, vasculitis, and watershed infarction from cardiac arrest, among others.
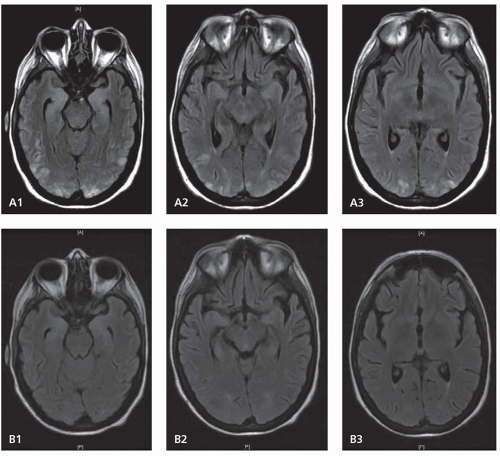 FIGURE 43.1 Magnetic resonance FLAIR image of posterior reversible encephalopathy syndrome on admission (A) and 2 weeks after stopping inciting medication (B). |
Call-Fleming syndrome, thunderclap headache-associated vasoconstriction, postpartum angiopathy, migraine angiitis, and cerebral vasospasm caused by cocaine, amphetamines, sumatriptan, and other serotonergic and sympathomimetic drugs.
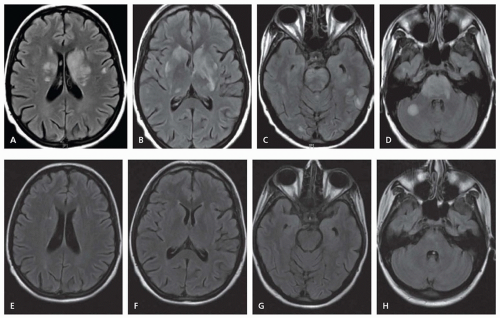 FIGURE 43.2 FLAIR images of posterior reversible encephalopathy syndrome presenting with prominent brain stem involvement (A-D). Nine days later, the lesions had significantly resolved (E-H). |
approximately 20% of patients at some point during the course of the illness, either alone or in combination. The focal deficits usually last minutes to hours but in some cases are persistent and associated with focal infarction. Blood pressure surges occur in 40% of patients; it is unclear if these elevations are related to the primary condition or are a reaction to pain or neurologic injury. Rupture or reperfusion injuries involving small leptomeningeal arteries may cause convexity SAHs.
TABLE 43.2 Etiologies of Posterior Reversible Encephalopathy Syndrome | ||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
TABLE 43.3 Precipitants of Reversible Cerebral Vasoconstriction Syndrome | ||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||
angiography. By the end of the clinical course, 80% of patients eventually develop lesions on MRI. Common findings include convexity SAH, small discrete intracerebral hemorrhages, and infarcts.
TABLE 43.4 Summary of Critical Elements for the Diagnosis of Reversible Cerebral Vasoconstriction Syndrome | |||||||
|---|---|---|---|---|---|---|---|
|
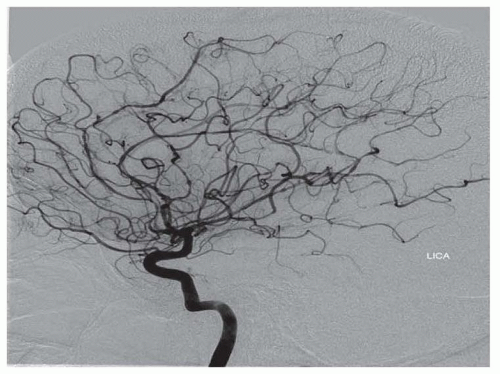 FIGURE 43.3 Multifocal beading of the cerebral vasculature, characteristic of reversible cerebral vasoconstriction syndrome. (From Neil WP, Dechant V, Urtecho J. Pearls and oy-sters: reversible cerebral vasoconstriction syndrome precipitated by ascent to high altitude. Neurology. 2011;76:e7-e9.) |
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


