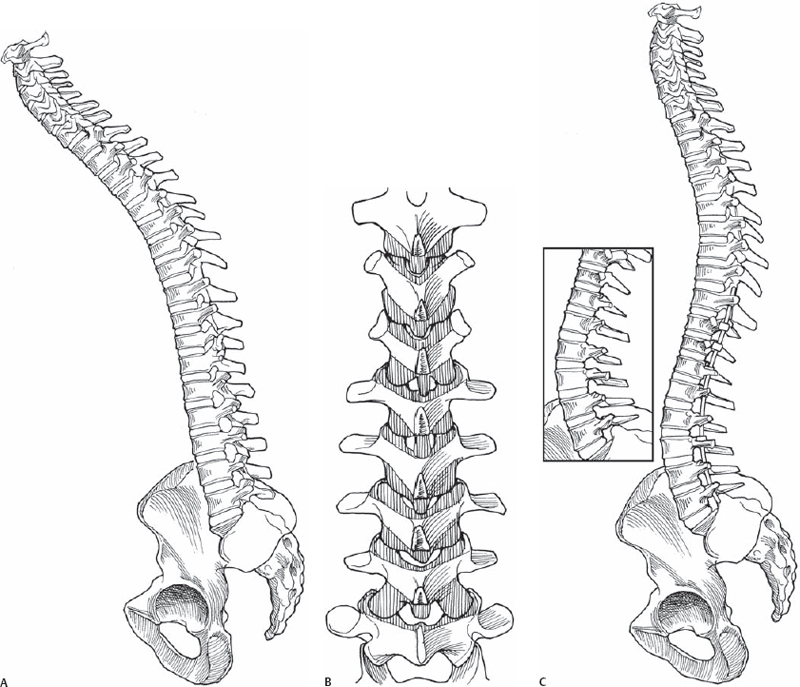
62 Stephen L. Ondra and Brian A. O’Shaughnessy Although modern spinal implants enable the surgeon to exert powerful force on the spine in the correction of deformity, the limiting factor remains the bone-metal interface. As a result, there is a limit to the force that can be applied to the spine. Osteotomies are the primary tool in the surgical armamentarium by which the surgeon can introduce mobility into the spinal column, thereby decreasing the forces required to obtain a correction. Osteotomies also alter the anatomy of the spinal column, and when combined with spinal implants and interbody devices, enable the surgeon to manipulate the axis of rotation to more effectively obtain the desired correction. The three most commonly implemented osteotomies in deformity surgery are the Smith-Petersen osteotomy, pedicle subtraction osteotomy, and vertebral column resection osteotomy. The choice of osteotomy is dependent on the goals of the procedure, the correction requirements, the native bone quality of the patient, and the anatomic variations that may be present. Each of the osteotomy techniques has specific advantages as well as inherent limitations. They can be used individually or in combination to achieve the desired correction. In theory, the Smith-Petersen osteotomy offers up to 10 degrees of correction per level; however, 3 to 7 degrees per level is more commonly achieved. It can be performed at any level in the thoracolumbar spine and is best accomplished at a level where there is a disk that is not ankylosed. The taller the disk, the more effective the osteotomy, as this technique requires posterior osteotomy closure and simultaneous anterior opening. The pedicle subtraction osteotomy, a more powerful technique that hinges on the anterior column and involves middle and posterior column shortening, can reliably achieve between 30 and 40 degrees of correction at a single level. A vertebral column resection procedure, an extension of the pedicle subtraction technique, typically yields a bit more correction than a standard pedicle subtraction osteotomy due to the distance and height of the anterior pivot, which places the correction arc point anterior to the vertebral body. The indications for each of these osteotomy techniques include fixed segmental kyphosis or globally positive sagittal imbalance. The Smith-Petersen osteotomy requires a mobile anterior column, which is not always the case. A pedicle subtraction osteotomy, by contrast, does not possess the same limitation because the bony resection is carried through into the anterior column. Although a pedicle subtraction osteotomy is commonly performed for fixed sagittal correction, it can also be used for coronal correction or combined sagittal-coronal correction. The pedicle subtraction osteotomy can also be utilized in nonfixed deformity if other techniques will not give the needed correction. A vertebral column resection procedure, the most powerful osteotomy technique, is particularly valuable in the setting of sharp, angular deformities. The choice of osteotomy is based on the bone quality, patient needs, local anatomy, pathology, and the amount of correction needed. The desired correction is often either estimated or calculated by doing cumbersome radiographic cutouts. We have developed a method that allows rapid, easy, and precise mathematical calculation of the degrees of correction needed in any plane. This has translated into the operating room by allowing the degrees of correction to the osteotomy to be translated into millimeters of bony resection throughout the osteotomy. Our method, which takes advantage of simple trigonometry, has had a high level of correlation between the calculated degrees, the bony resection based on these parameters, and the clinical result. The distance from the planned osteotomy to C7 is measured. The distance from C7 to the S1 plumb line on a standing 36-inch film is then measured. This establishes a right triangle and a simple trigonometric calculation is performed: (Opposite/Adjacent) -1 = Angle. In this case it is (C7 – S1 Plumb Line Distance/ Osteotomy to C7 Distance) -1 = Angle Needed for Correction. Once the degrees needed for correction are known, the surgeon can make the decision as to what single osteotomy or combination of osteotomies is needed to accomplish the planned correction based on the expected correction with each type of osteotomy and the unique patient characteristics that may enhance or limit an osteotomy correction. For instance, if the surgeon knows that 45 degrees of correction are needed, it is unlikely to be achieved by three or four Smith-Petersen osteotomies. More likely, a single pedicle subtraction coupled with one or two Smith-Petersen osteotomies would be adequate. This type of calculation and information enables the surgeon to develop a comprehensive surgical plan that realistically achieves the goals of correction. The patient is positioned prone on a radiolucent frame with four to six posts allowing the abdomen to be free of pressure. The patient is typically “built up” on a chest pad so as to render the lumbar spine as lordotic as possible. Particularly when there is a mobile anterior column, patients often sustain a reasonable degree of correction simply by proper positioning. In general, it should be noted that stainless steel rods are preferred in all the osteotomy correction techniques as microfractures in titanium is more common with large bends and can lead to rod failure at an increased rate. In performing the Smith-Petersen osteotomy, we often initially prepare the screw or other implant sites, but we do not actually place the implant until just prior to the osteotomy closure. A Gelfoam product can be used to minimize bleeding until the implant is placed. This approach has the advantage of allowing screw hole placement and preparation while all anatomic landmarks are present. It also allows for much of the work to be done while minimizing the time that the osteotomy is present, as this may be a source of blood loss. Not placing the screw until the osteotomy is done prevents the screw head from getting in the way and decreasing the efficiency of the bone removal at the superior facet. The most important aspect of this osteotomy is removal of the superior facet. The osteotomy is begun by using an osteotome to resect the inferior facet the desired number of millimeters. A drill is then utilized to create a chevron-like resection of the inferior and superior facet complex and the inferior edge of the superior lamina of the osteotomy level. The ligamentum flavum is then resected to expose the dura (Fig. 62.1A,B). Gelfoam is used to decrease bleeding. Once all osteotomies are completed, the pedicle screws or other implants are placed. Closure is achieved by compression, postural effects, table manipulation, or some combination of these (Fig. 62.1C).
Posterior Smith-Petersen, Pedicle Subtraction, and Vertebral Column Resection Osteotomy Techniques
Description
Expectations
Indications and Contraindications
Special Considerations
Tips, Pearls, and Lessons Learned
Key Procedural Steps
Smith-Petersen Osteotomy
Related posts:
 Anterior Thoracic and Thoracolumbar Plating Techniques
Anterior Thoracic and Thoracolumbar Plating Techniques
 Anterior Cervical Corpectomy
Anterior Cervical Corpectomy
 Minimally Invasive Posterior Surgical Approaches to the Lumbar Spine Through Tubular Retractors
Minimally Invasive Posterior Surgical Approaches to the Lumbar Spine Through Tubular Retractors
 Open Lumbar Microscopic Diskectomy
Open Lumbar Microscopic Diskectomy
 Spondylolysis Repair (Pars Interarticularis Repair)
Spondylolysis Repair (Pars Interarticularis Repair)
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


