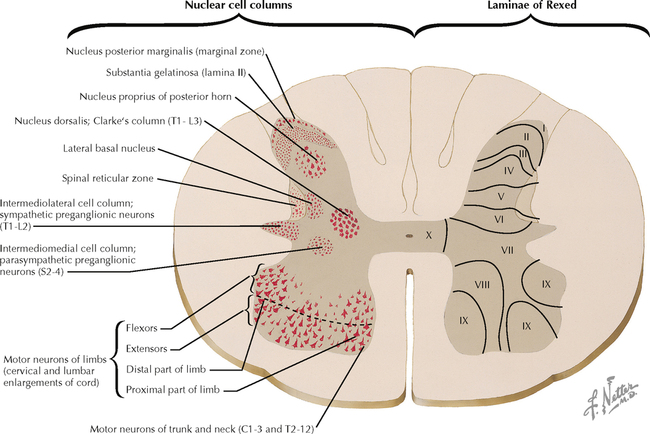
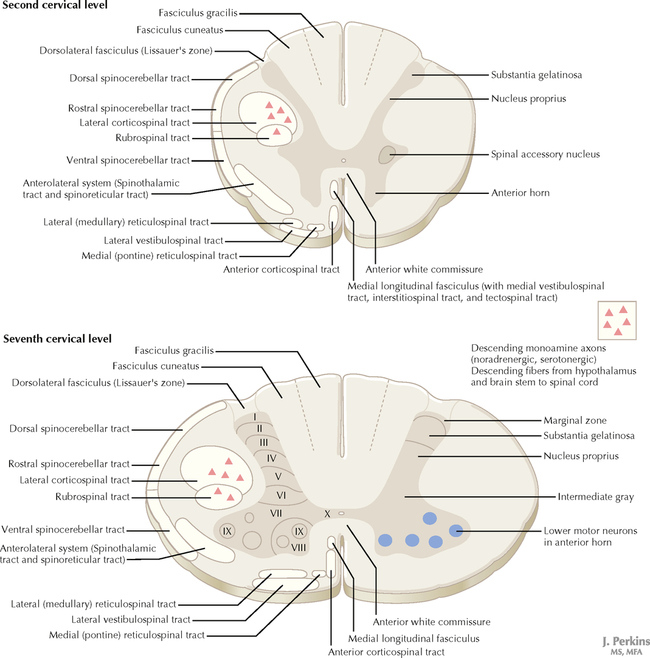
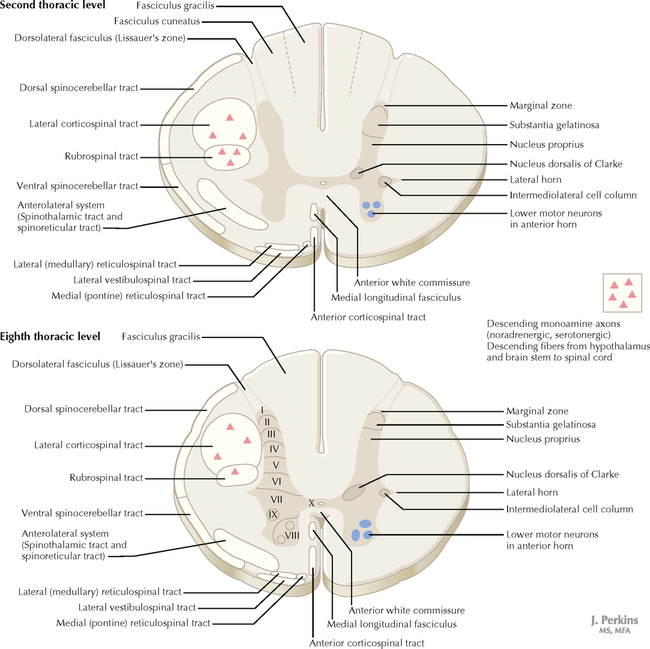
10 SPINAL CORD 10.1. Cytoarchitecture of the Spinal Cord Gray Matter 10.2. Spinal Cord Levels: Cervical, Thoracic, Lumbar, and Sacral 10.3. Spinal Cord Levels: Cervical, Thoracic, Lumbar, and Sacral 10.4. Spinal Cord Levels: Cervical, Thoracic, Lumbar, and Sacral 10.5. Spinal Cord Levels: Cervical, Thoracic, Lumbar, and Sacral 10.6. Spinal Cord Levels: Cervical, Thoracic, Lumbar, and Sacral 10.7. Spinal Cord Lower Motor Neuron Organization and Control 10.8. Spinal Somatic Reflex Pathways 10.9. Muscle and Joint Receptors and Muscle Spindles 10.10. The Muscle Stretch Reflex and Its Central Control via Gamma Motor Neurons 10.1 CYTOARCHITECTURE OF THE SPINAL CORD GRAY MATTER The spinal cord gray matter is located centrally in the interior of the spinal cord in a butterfly pattern. The gray matter is subdivided into three horns: (1) the dorsal horn, a site of major sensory processing; (2) the intermediate gray with a lateral horn, a site where preganglionic sympathetic (thoracolumbar) and parasympathetic (sacral) neurons reside and where interneuronal processing occurs; and (3) the ventral horn, a site where lower motor neurons (LMNs) reside and where converging reflex and descending control of LMNs occurs. Neuronal cell groups appear homogeneous in some regions of gray matter, intermixed with a presence of some discrete nuclei (e.g., Clarke’s nucleus, substantia gelatinosa). Laminae of Rexed, an alternative system of cytoarchitectural classification established in the 1950s, subdivides the spinal cord gray matter into ten laminae. This system is used extensively for the dorsal horn and the intermediate gray, laminae I–VII, particularly in conjunction with anatomical details of nociceptive processing and for some reflex and cerebellar processing. Although these laminae have distinctive characteristics at each segmental level, they show some similarities across segmental levels. The absolute amount of spinal cord gray is more extensive in the cervical and lumbosacral enlargements of the spinal cord, which correspond to zones associated with limb innervation, than it is in upper cervical, thoracic, and sacral regions. CLINICAL POINT Classical descriptions of secondary sensory processing in the spinal cord describe neurons of lamina I (marginal zone) and lamina V of the dorsal horn as cells of origin for crossed projections into the spinothalamic/anterolateral system for the processing of pain and temperature sensation (protopathic modalities). Primary sensory large-diameter axons, carrying information about fine discriminative touch, vibratory sensation, and joint position sense (epicritic modalities), enter through the dorsal root entry zone and travel rostrally into the dorsal column system, bypassing synapses in the spinal cord; these axons terminate in their secondary sensory nuclei, gracilis and cuneatus, in the caudal medulla. According to this scheme, pure dorsal column lesions should result in the total loss of epicritic sensation on the ipsilateral side of the body below the level of the lesion. However, such lesions result in diminution of these epicritic sensations or in the inability to discriminate vibratory sensations of different frequencies, but not in the total loss of these modalities. Only with additional damage to the dorsolateral part of the lateral funiculus is the profound loss of epicritic sensation observed. This is because additional dorsal horn neurons receive primary sensory input related to epicritic sensation and send ipsilateral projections into the dorsolateral funiculus, providing additional contributions to lemniscal processing of fine discriminative modalities. 10.2 SPINAL CORD LEVELS: CERVICAL, THORACIC, LUMBAR, AND SACRAL The organization of the gray matter into laminae of Rexed is retained throughout the spinal cord. The dorsal and ventral horns are larger and wider at levels of the cervical and lumbosacral enlargements. The lateral horn is present from L1 to T2. Some nuclei are found only in circumscribed regions, such as the intermediolateral cell column with preganglionic sympathetic neurons (T1–L2 lateral horn); Clarke’s nucleus (C8–L2); and the parasympathetic preganglionic nucleus (S2–S4). The white matter increases in absolute amount from caudal to rostral. The dorsal columns contain only fasciculus gracilis below T6; fasciculus cuneatus is added laterally above T6. The spinothalamic/spinoreticular anterolateral system increases from caudal to rostral. The descending upper motor neuron (UMN) pathways diminish from rostral to caudal. The lateral corticospinal pathway loses more than half of its axons as they synapse in the cervical segments; this tract then diminishes in size as it extends caudally. 10.3 SPINAL CORD LEVELS: CERVICAL, THORACIC, LUMBAR, AND SACRAL CLINICAL POINT Only gold members can continue reading. Log In or Register to continue Share this:Click to share on Twitter (Opens in new window)Click to share on Facebook (Opens in new window) Related Related posts: VENTRICLES AND THE CEREBROSPINAL FLUID MOTOR SYSTEMS NEURONS AND THEIR PROPERTIES AUTONOMIC-HYPOTHALAMIC-LIMBIC SYSTEMS TELENCEPHALON PERIPHERAL NERVOUS SYSTEM Stay updated, free articles. Join our Telegram channel Join Tags: Netters Atlas of Neuroscience with STUDENT CONSULT Online Access Jun 4, 2016 | Posted by admin in NEUROLOGY | Comments Off on SPINAL CORD Full access? Get Clinical Tree
10 SPINAL CORD 10.1. Cytoarchitecture of the Spinal Cord Gray Matter 10.2. Spinal Cord Levels: Cervical, Thoracic, Lumbar, and Sacral 10.3. Spinal Cord Levels: Cervical, Thoracic, Lumbar, and Sacral 10.4. Spinal Cord Levels: Cervical, Thoracic, Lumbar, and Sacral 10.5. Spinal Cord Levels: Cervical, Thoracic, Lumbar, and Sacral 10.6. Spinal Cord Levels: Cervical, Thoracic, Lumbar, and Sacral 10.7. Spinal Cord Lower Motor Neuron Organization and Control 10.8. Spinal Somatic Reflex Pathways 10.9. Muscle and Joint Receptors and Muscle Spindles 10.10. The Muscle Stretch Reflex and Its Central Control via Gamma Motor Neurons 10.1 CYTOARCHITECTURE OF THE SPINAL CORD GRAY MATTER The spinal cord gray matter is located centrally in the interior of the spinal cord in a butterfly pattern. The gray matter is subdivided into three horns: (1) the dorsal horn, a site of major sensory processing; (2) the intermediate gray with a lateral horn, a site where preganglionic sympathetic (thoracolumbar) and parasympathetic (sacral) neurons reside and where interneuronal processing occurs; and (3) the ventral horn, a site where lower motor neurons (LMNs) reside and where converging reflex and descending control of LMNs occurs. Neuronal cell groups appear homogeneous in some regions of gray matter, intermixed with a presence of some discrete nuclei (e.g., Clarke’s nucleus, substantia gelatinosa). Laminae of Rexed, an alternative system of cytoarchitectural classification established in the 1950s, subdivides the spinal cord gray matter into ten laminae. This system is used extensively for the dorsal horn and the intermediate gray, laminae I–VII, particularly in conjunction with anatomical details of nociceptive processing and for some reflex and cerebellar processing. Although these laminae have distinctive characteristics at each segmental level, they show some similarities across segmental levels. The absolute amount of spinal cord gray is more extensive in the cervical and lumbosacral enlargements of the spinal cord, which correspond to zones associated with limb innervation, than it is in upper cervical, thoracic, and sacral regions. CLINICAL POINT Classical descriptions of secondary sensory processing in the spinal cord describe neurons of lamina I (marginal zone) and lamina V of the dorsal horn as cells of origin for crossed projections into the spinothalamic/anterolateral system for the processing of pain and temperature sensation (protopathic modalities). Primary sensory large-diameter axons, carrying information about fine discriminative touch, vibratory sensation, and joint position sense (epicritic modalities), enter through the dorsal root entry zone and travel rostrally into the dorsal column system, bypassing synapses in the spinal cord; these axons terminate in their secondary sensory nuclei, gracilis and cuneatus, in the caudal medulla. According to this scheme, pure dorsal column lesions should result in the total loss of epicritic sensation on the ipsilateral side of the body below the level of the lesion. However, such lesions result in diminution of these epicritic sensations or in the inability to discriminate vibratory sensations of different frequencies, but not in the total loss of these modalities. Only with additional damage to the dorsolateral part of the lateral funiculus is the profound loss of epicritic sensation observed. This is because additional dorsal horn neurons receive primary sensory input related to epicritic sensation and send ipsilateral projections into the dorsolateral funiculus, providing additional contributions to lemniscal processing of fine discriminative modalities. 10.2 SPINAL CORD LEVELS: CERVICAL, THORACIC, LUMBAR, AND SACRAL The organization of the gray matter into laminae of Rexed is retained throughout the spinal cord. The dorsal and ventral horns are larger and wider at levels of the cervical and lumbosacral enlargements. The lateral horn is present from L1 to T2. Some nuclei are found only in circumscribed regions, such as the intermediolateral cell column with preganglionic sympathetic neurons (T1–L2 lateral horn); Clarke’s nucleus (C8–L2); and the parasympathetic preganglionic nucleus (S2–S4). The white matter increases in absolute amount from caudal to rostral. The dorsal columns contain only fasciculus gracilis below T6; fasciculus cuneatus is added laterally above T6. The spinothalamic/spinoreticular anterolateral system increases from caudal to rostral. The descending upper motor neuron (UMN) pathways diminish from rostral to caudal. The lateral corticospinal pathway loses more than half of its axons as they synapse in the cervical segments; this tract then diminishes in size as it extends caudally. 10.3 SPINAL CORD LEVELS: CERVICAL, THORACIC, LUMBAR, AND SACRAL CLINICAL POINT Only gold members can continue reading. Log In or Register to continue Share this:Click to share on Twitter (Opens in new window)Click to share on Facebook (Opens in new window) Related Related posts: VENTRICLES AND THE CEREBROSPINAL FLUID MOTOR SYSTEMS NEURONS AND THEIR PROPERTIES AUTONOMIC-HYPOTHALAMIC-LIMBIC SYSTEMS TELENCEPHALON PERIPHERAL NERVOUS SYSTEM Stay updated, free articles. Join our Telegram channel Join Tags: Netters Atlas of Neuroscience with STUDENT CONSULT Online Access Jun 4, 2016 | Posted by admin in NEUROLOGY | Comments Off on SPINAL CORD Full access? Get Clinical Tree