Fig. 34.1
14-year-old with a prominent gibbus and kyphectomy deformity (Reprinted from Furderer et al. [7] with permission from Springer Science)

Fig. 34.2
Lateral radiograph demonstrating severe kyphotic deformity (Reprinted from Furderer et al. [7] with permission from Springer Science)

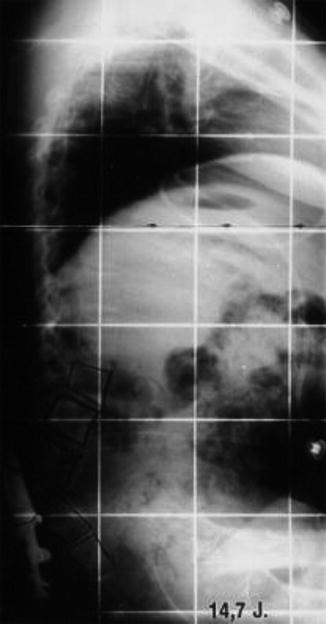
Fig. 34.4
Lateral radiographs after correction of kyphotic deformity (Reprinted from Furderer et al. [7] with permission from Springer Science)
One of the most studied kyphectomy surgical procedures is vertebral resection with modified Luque fixation (resection kyphectomy). As shown by Lindseth in 1979, in addition to vertebral resection of the apex of the kyphotic deformity, resection of 1.5–2.5 vertebral bodies cephalad to the apical vertebra must also be performed to best correct the lumbar kyphosis and distal rigid compensatory thoracic lordosis [5]. The extent of resection must extend to the lordotic segment. One of the often-cited limitations of this procedure includes the potential inability to allow for complete preservation of the dural sac and subsequent potential life-threatening postoperative complications that may occur such as increased epidural bleeding and specifically acute hydrocephalus [16, 17]. Winston et al. also reported a case of sudden death from elevated intracranial pressure presumably due to CSF flow changes after ligation of the thecal sac [18]. Additionally, this procedure leads to vertebral shortening and an indirect reduction of tension on the spinal cord [3].
Another kyphectomy surgical technique is subtraction (decancellation) vertebrectomy. Conceptually, the decancellation kyphectomy technique is a lordosing intravertebral apical osteotomy over multiple lumbar levels. This procedure obviates the need to perform a cordotomy and the resulting associated morbidities of cerebrospinal fluid flow problems such as meningitis and acute hydrocephalus [3]. Additionally, this method is not a complete resection of a significant portion of the spinal column, allowing for preservation of spinal height. The lordosing kyphectomy is tethered along the length of the anterior longitudinal ligament, thus avoiding tension on neurovascular structures. The advantages of this procedure when compared to the vertebral resection include a satisfactory sagittal correction, preservation of the dural sac leading to fewer shunt complications, less blood loss, and decreased operative time [16]. The preferred age for surgery seems to be between 2 and 5 years of age, when the anteroposterior diameter reaches a 25 mm minimum [3].
With either the resection kyphectomy or decancellation kyphectomy, stable instrumentation is required to stabilize the osteotomies and sagittal correction, prevent recurrence, and allow for seating stability. The pelvis or sacrum should be included distally—in most instances—to prevent lumbosacral sagittal plane deformity. Additionally, the instrumentation must correct the developmental thoracic lordosis by including the thoracic spine to the level of T4–T6. A wide range of long-term results has been generated when performing a resection kyphectomy using different instrumentation techniques including the use of Harrington rods; plate fixation; Luque rods; combinations of cables, hooks, and wires; the Galveston technique; Dunn-McCarthy fixation; or the Warner and Fackler technique [14, 19–25]. However, the current consensus is that segmental posterior spinal instrumentation with inclusion of the sacropelvis is necessary to attain and maintain sagittal correction, which, again, can be achieved with multiple different techniques [8, 16, 17, 19, 20, 22, 25, 26].
34.3.2 Surgical Technique Specific
34.3.2.1 Vertebral Resection Kyphectomy Technique
The procedure is performed with the patient under general anesthesia, prone positioning, a radiolucent operating table, and a frame or chest rolls. A posterior midline longitudinal incision is used and developed through the area of previous closure. If a tissue expansion procedure has been completed, the tissue expanders are removed at the conclusion and closure of the case. The thoracic paraspinal muscles are subperiosteally dissected from the thoracic posterior spinal elements. At the lumbosacral junction, the dural sac is dissected, and the proximal stump is oversewn. Evidence of a functioning shunt must be determined preoperatively. Of note, the visualization of cerebrospinal fluid during this portion of the procedure precludes closure of the neural plaque in fear of precipitating acute hydrocephalus [22]. Then, the dural sac is retracted proximal to the osteotomy site.
Dissection is performed laterally and anteriorly around the kyphosis in order to access the sinus of the kyphosis. The kyphectomy is then performed via vertebral excision of the proximal aspect of the apical vertebra and one to two vertebral bodies cephalad to the kyphotic apex [5].
Modified segmental instrumentation using the Luque technique as outlined by McCall may be utilized to correct and stabilize the kyphectomy (Figs. 34.5, 34.6, and 34.7) [22]. Contoured Luque rods are brought through the S1 foramen bilaterally, with the distal ends lying on the anterior aspect of the sacrum. The distal ends of the Luque rods are bent in accordance with the patient’s sacral inclination, approximately 20–40°. A cross-link is placed distally near the sacral foramen to prevent rod migration and rotation. The rods are placed just medial to the lateral masses at the level of the osteotomy site and subsequently wired to the higher-level thoracic lamina sequentially starting at T4, progressively reducing the osteotomy site and creating more rigid fixation. The osteotomy site is augmented with bone from the vertebrectomy to perform a local arthrodesis [22].

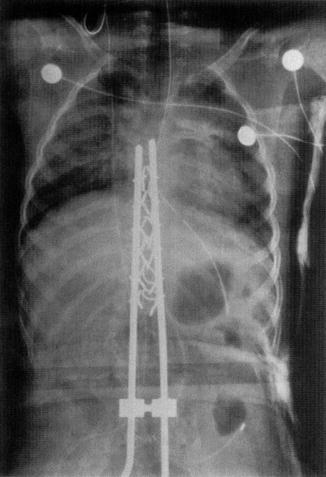
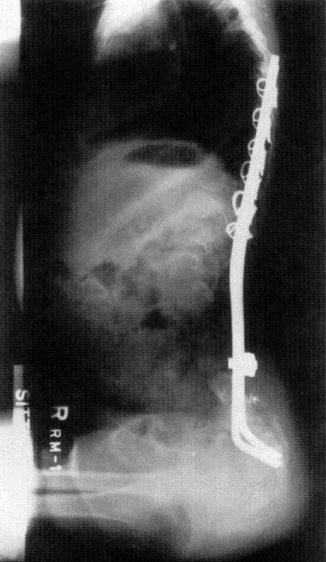
Fig. 34.5
5-year-old child with kyphotic deformity (Reprinted from McCall [22] with permission from Wolters Kluwer Health)
Fig. 34.6
Postoperative AP image showing rod construct (Reprinted from McCall [22] with permission from Wolters Kluwer Health)
Fig. 34.7
6-month postoperative x-ray of same patient with demonstration of kyphotic reduction with Luque rods (Reprinted from McCall [22] with permission from Wolters Kluwer Health)
34.3.2.2 Subtraction (Decancellation) Kyphectomy Technique: Pedicle Subtraction Osteotomy
The operation is performed with the patient under general anesthesia and prone positioning using a radiolucent operating table and frame or chest rolls. The procedure is performed through a posterior midline incision. The laminar bars are subperiosteally exposed laterally and medially. The dorsal laminar bar overlying each respective neuroforamen is resected for isolation of each pedicle needed for decancellation. The thecal sac and nerve roots are mobilized medially in the subperiosteal plane. The pedicle is entered with a curette from one side, and the cancellous bone is progressively evacuated from the vertebral body to the midline. Subsequently, this canal is packed and the procedure is repeated on the contralateral side, resulting in a cortical shell of vertebral body. A fine curette is used to etch a line in the anterior cortex of the vertebral body from pedicle to pedicle. The osteotomy will close or hinge on this line. This decancellation procedure is then repeated over contiguous levels from caudad to cephalad, usually beginning at L4 and progressing to L1. A correction of 45° per vertebral level can be expected with restitution of lumbar lordosis, thoracic kyphosis, and sagittal balance [3].
Stable instrumentation is required to stabilize the multilevel osteotomies and correction, prevent recurrence, and allow for seating stability and long-term stability. Again, the pelvis or sacrum must be included distally to prevent lumbosacral sagittal plane deformity. Additionally, the instrumentation must correct the rigid developmental thoracic lordosis by including the thoracic spine to the level of T4–T6. Instrumentation techniques include posterior stabilization with neutral or sagittally contoured, paired rods; segmental thoracic hooks or sublaminar wires; lumbosacral pedicle screw fixation with intrasacral distal rod insertion (Roger Jackson technique); and limited arthrodesis at the lumbosacral fixation points allowing growth proximally [16]. Furthermore, a growing construct can be attempted by extraperiosteal dissection for thoracic lamina exposure, limited lumbosacral arthrodesis, preservation of cartilaginous end plates at the decancellated levels, and utilization of segmental thoracic hooks, sublaminar wires, or cables (Fig. 34.8) [3].
Fig. 34.8
(a) Postoperative AP image of subtraction kyphectomy and instrumentation. A growth construct is placed proximally to allow for column growth with arthrodesis only in the lumbosacral region. (b) Postoperative lateral image of subtraction kyphectomy and instrumentation. Lumbosacral fixation includes L5 and S1 pedicle screw fixation and intra-alar rod insertion. Rod contour is normal sagittal profile
34.3.3 Results
The results from the resection kyphectomy have varied dependent on the form of instrumentation. However, from these prior studies, it has been agreed upon that segmental spinal instrumentation with sacral fixation is important to obtain and maintain kyphectomy correction and stability.
Sharrard (1968) and Lindseth (1979) first described resection of vertebral bodies for treatment of kyphosis, which required significant postoperative immobilization [5, 27]. Since that time though, many different techniques for resection kyphectomy have been developed. Heydemann and Gillespie reported improved results using sublaminar wiring at the osteotomy site supplemented with Luque rods placed anterior to the sacrum distally, which no longer require postoperative external immobilization [20]. They showed a kyphosis correction from 124° to 33° postoperatively which was maintained at final follow-up. McCarthy in 1989 concluded that long posterior spinal fusion with Luque rod instrumentation achieved the best outcomes; and the Dunn McCarthy modification involved placement of Luque rods into the sacral ala [28]. Warner and Fackler also modified sacral anchoring and achieved improved correction and stability [25]. Their technique has since been a popular treatment method in institutions around the world. Lintner and Lindseth demonstrated that resection kyphectomy resulted in a mean correction to 40° kyphosis postoperatively and 62° at follow-up [4]. This also demonstrated how limited fixation might lead to loss of correction over a period of time as 34 of their 39 patients had a partial loss of correction. Huang and Lubicky illustrated that resection kyphectomy and posterior spinal instrumentation using Luque rods resulted in a mean correction of 21° postoperatively and 23.7° at follow-up [17]. McCall in 1998 showed a mean correction of 15° kyphosis postoperatively and 20° of kyphosis at follow-up assessment with a mean postoperative correction of 91° [22]. Overall, these studies have demonstrated mean postoperative corrections of 84–94 % and average final 5 year retained corrections of 81–93 % performing resection kyphectomies with rigid segmented fixation with Luque rods [17, 20, 22].
Related posts:
 Other Neuromuscular Diseases
Other Neuromuscular Diseases
 Clinical Examination and Associated Comorbidities of Early Onset Scoliosis
Clinical Examination and Associated Comorbidities of Early Onset Scoliosis
 Revision Spine Surgery in the Growing Child
Revision Spine Surgery in the Growing Child
 Imaging of the Growing Spine
Imaging of the Growing Spine
 Growth-Guided Instrumentation: Shilla Procedure
Growth-Guided Instrumentation: Shilla Procedure
 Plate-Rod System in the Management for Progressive Scoliosis in Growing Children
Plate-Rod System in the Management for Progressive Scoliosis in Growing Children
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


