Traumatic brain injury (TBI) is a modern scourge of industrialized society. It is a major cause of death, especially in young adults, and a major cause of disability. The costs in human misery and dollars are exceeded by few other conditions.
More than 2 million patients with head injuries are seen annually in U.S. emergency rooms, and 25% of these patients are admitted to a hospital. In general, total combined rates for TBI-related emergency department (ED) visits, hospitalizations, and deaths have increased over the past decade. Almost 10% of all deaths in the United States are caused by injury, and about half of the traumatic deaths involve the brain. In the United States, a head injury occurs every 7 seconds and a death every 5 minutes. About 200,000 people are killed or permanently disabled annually as a result.
Brain injuries occur at all ages, but the peak is in young adults between the ages of 15 and 24 years. Head injury is the leading cause of death among people younger than the age of 24 years. There is, however, a trend toward an increase of mortality rates from TBI among populations aged older than 65 years over the past decade. It is anticipated that this trend will continue as the overall population ages. Men are affected three or four times as often as women. The major causes of brain injury differ in different parts of the United States; in all areas, motor vehicle accidents are prominent, and in metropolitan areas, personal violence is prevalent.
PATHOBIOLOGY
SKULL FRACTURES
Skull fractures may be divided into linear, depressed, or comminuted types. If the scalp is lacerated over the fracture, it is considered an open or compound fracture. Skull fractures are important markers of a possibly serious injury but rarely cause problems by themselves; prognosis depends more on the nature and severity of injury to the brain than on the severity of injury to the skull.
About 80% of fractures are linear. They occur most commonly in the temporoparietal region, where the skull is thinnest. Detection of a linear fracture often raises the suspicion of serious brain injury, but computed tomography (CT) in most patients is otherwise normal. Nondisplaced, linear skull fractures generally do not require surgery and can be managed conservatively.
In depressed fracture of the skull, one or more fragments of bone are displaced inward, compressing the underlying brain. In comminuted fracture, there are multiple, shattered bone fragments, which may or may not be displaced. In 85% of cases, depressed fractures are open (or “compound”) and liable to become infected or leak cerebrospinal fluid (CSF). Even when closed, most depressed or comminuted fractures require surgical exploration for debridement, elevation of bone fragments, and repair of dural lacerations. The underlying brain is injured in many cases. In some patients, depressed skull fractures are associated with tearing, compression, or thrombosis of underlying venous dural sinuses.
Basilar skull fractures may be linear, depressed, or comminuted. They are frequently missed by standard skull x-rays and are best identified by CT bone windows. There may be associated cranial nerve injury or a dural tear adjacent to the fracture site, which may lead to delayed meningitis if bacteria enter the subarachnoid space. Signs that lead the physician to suspect a fracture of the petrous portion of the temporal bone include hemotympanum or tympanic perforation, hearing loss, CSF otorrhea, peripheral facial nerve weakness, or ecchymosis of the scalp overlying the mastoid process (Battle sign). Anosmia, bilateral periorbital ecchymosis, and CSF rhinorrhea suggest possible fracture of the sphenoid, frontal, or ethmoid bones.
CEREBRAL CONCUSSION AND AXONAL-SHEARING INJURY
Loss of consciousness at the moment of impact is caused by acceleration-deceleration movements of the head, which result in the stretching and shearing of axons. When the alteration of consciousness is brief (e.g., <6 hours), the term concussion is used. These patients may be completely unconscious or remain awake but appear dazed; most recover within seconds or minutes, rather than hours, and some have retrograde or anterograde amnesia surrounding the event.
The mechanism by which concussion leads to loss of consciousness is believed to be transient functional disruption of the reticular activating system caused by rotational forces on the upper brain stem. Experimentally, sudden and violent head rotation may produce concussion without impact to the head. Most patients with concussion have normal CT or magnetic resonance imaging (MRI) findings because concussion results from physiologic, rather than structural, injury to the brain. Only 5% of patients who have sustained a concussion and are otherwise intact have an intracranial hemorrhage on CT.
The term diffuse axonal injury (DAI) is applied to traumatic coma lasting more than 6 hours. In these cases, when no other cause of coma is identified by CT or MRI, it is presumed that widespread microscopic and macroscopic axonal-shearing injury has occurred. Coma of 6 to 24 hours duration is deemed mild DAI; coma lasting more than 24 hours is considered moderate or severe DAI, depending on the absence or presence of brain stem signs, such as decorticate or decerebrate posturing (Table 46.1).
Autonomic dysfunction (e.g., hypertension, hyperhidrosis, hyperpyrexia) is common in patients with acute severe DAI and may reflect brain stem or hypothalamic injury. Patients may remain unconscious for days, months, or years, and those who recover may be left with severe cognitive and motor impairment, including spasticity and ataxia. DAI is considered the single most important cause of persistent disability after traumatic brain damage.
TABLE 46.1 Clinical Characteristics and Outcome of Diffuse Brain Injuries
Diffuse Axonal Injury
Mild Concussion
Cerebral Contusion
Mild
Moderate
Severe
Loss of consciousness
None
Immediate
Immediate
Immediate
Immediate
Length of unconsciousness
None
<6 h
6-24 h
>24 h
Days to weeks
Decerebrate posturing
None
None
Rare
Occasionally
Present
Posttraumatic amnesia
Minutes
Minutes to hours
Hours
Days
Weeks
Memory deficit
None
Mild
Mild to moderate
Mild to moderate
Severe
Motor deficits
None
None
None
Mild
Severe
Outcome at 3 mo (%)
Good recovery
100
95
63
38
15
Moderate deficit
0
5
15
21
13
Severe deficit
0
0
6
12
14
Vegetative
0
0
1
5
7
Death
0
0
15
24
51
Adapted from Gennarelli TA. Cerebral concussion and diffuse brain injuries. In: Cooper PR, ed. Head Injury. 3rd ed. Baltimore: Williams & Wilkins; 1993:140.
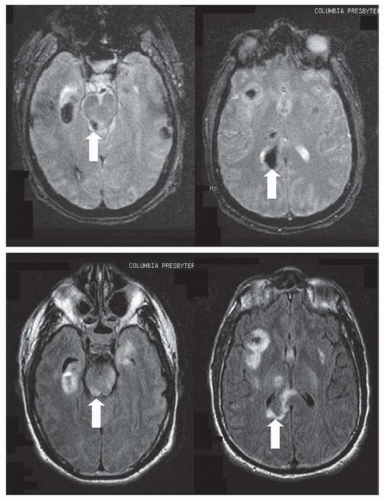
Axonal-shearing injury tends to be most severe in specific brain regions that are anatomically predisposed to maximal stress from rotational forces. Macroscopic tissue tears, best visualized by MRI, tend to occur in midline structures, including the dorsolateral midbrain and pons, posterior corpus callosum, parasagittal white matter, periventricular regions, and internal capsule. Microscopic damage occurs more diffusely, as manifested by axonal retraction bulbs throughout the white matter of the cerebral hemispheres. Prolonged loss of consciousness from DAI tends to be associated with bilateral, asymmetric, focal lesions of the midbrain tegmentum, a region densely populated with reticular activating system neurons. Small hemorrhages, known as gliding contusions, are sometimes associated with focal-shearing lesions (Fig. 46.1).
Axonal shearing is thought to initiate a dynamic sequence of pathologic events that evolve over days to weeks. Initially, injury causes physical transection of some neurons and internal axonal damage to many others. In both cases, the process of axoplasmic transport continues, and materials flow from the cell body to the site of damage. These materials accumulate and may lead to secondary axonal transection, with formation of a “retraction ball” from 12 hours to several days after the injury. Membrane channels may open to admit toxic levels of calcium. If the patient survives, MRI may demonstrate chronic atrophy of involved white matter tracts (wallerian degeneration) and gliosis.
BRAIN SWELLING AND CEREBRAL EDEMA
Brain swelling after head injury is a poorly understood phenomenon that may result from several different mechanisms. Posttraumatic brain swelling may result from cerebral edema (e.g., an increase in the content of extravascular brain water), an increase in cerebral blood volume (CBV) resulting from abnormal vasodilatation, or both. Cerebral edema may be further classified as cytotoxic, vasogenic, or interstitial (see Chapter 107). The swelling may be diffuse or focal, adjacent to a parenchymal or extradural hemorrhage, or related to contusion or infarction.
Brain swelling may follow any type of head injury. Curiously, the magnitude of swelling does not always correlate well with the severity of injury. In some cases, particularly in young people, severe diffuse brain swelling that may be fatal occurs minutes to hours after a minor concussion. Abnormal dilation of the cerebral blood vessels is thought to lead to increased CBV, hyperperfusion, and increased vascular permeability, resulting in secondary leakage of plasma and vasogenic cerebral edema. Cerebral blood flow studies indicate that after an initial period of hypoperfusion within the first 24 hours, hyperemia occurs in nearly all patients 1 to 3 days after severe head injury, followed less commonly by arterial vasospasm between days 4 and 7. Severe brain swelling may be related to local endothelial and microcirculatory dysfunction or from damage to cerebral vasomotor regulatory centers in the brain stem.
PARENCHYMAL CONTUSION AND HEMORRHAGE
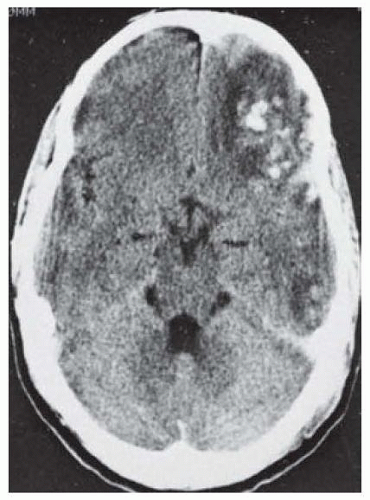
Cerebral contusions are focal parenchymal hemorrhages that result from scraping and bruising of the brain as it moves across the inner surface of the skull. The inferior frontal and temporal lobes, where brain tissue comes in contact with irregular protuberances at the base of the skull, are the most common sites of traumatic contusion (Fig. 46.2). Linear tears of the meninges or cerebral tissue, usually a result of cuts from the sharp edges of depressed skull fragments, are called lacerations.
Hemorrhagic contusions may occur at the site of a skull fracture but more often occur without a fracture and with the overlying pia and arachnoid left intact. In most patients, contusions are small and multiple. With lateral forces, contusions may occur at the site of the blow to the head (coup lesions) or at the opposite pole as the brain impacts on the inner table of the skull (contrecoup lesions). Contusions frequently enlarge over 12 to 24 hours, especially in the setting of coagulopathy. In some cases, contusions appear in delayed fashion 1 or more days after injury.
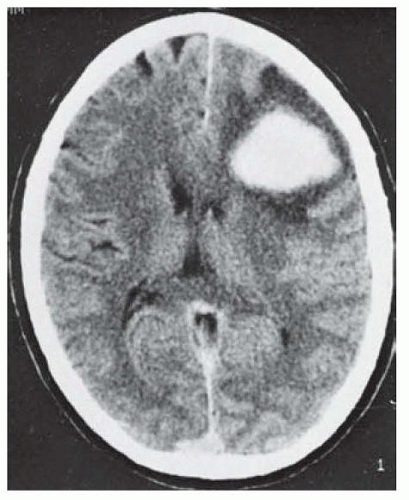
When rotational forces lead to tearing of small- or mediumsized vessels within the parenchyma, an intracerebral hematoma may occur (Fig. 46.3). Hematomas are focal collections of blood clots that displace the brain, in contrast to contusions, which resemble bruised and bloodied brain tissue (Fig. 46.4). Most parenchymal hematomas are located in the deep white matter, in contrast to contusions, which tend to be cortical.
FIGURE 46.1 Focal MRI findings characteristic of diffuse axonalshearing injury after neurotrauma. Top: Gradient echo (T2*) images demonstrating hemorrhagic lesions (gliding contusions) of the right dorsolateral midbrain and splenium of the corpus callosum. Bottom: FLAIR images showing edema in these regions.
FIGURE 46.2 Traumatic contusions. Axial noncontrast view demonstrates areas of contusion with small focal hemorrhages involving the lower poles of the left frontal and temporal lobes adjacent to the rough cranial vault. (Courtesy of Drs. S. K. Hilal, J. A. Bello, and T. L. Chi.)
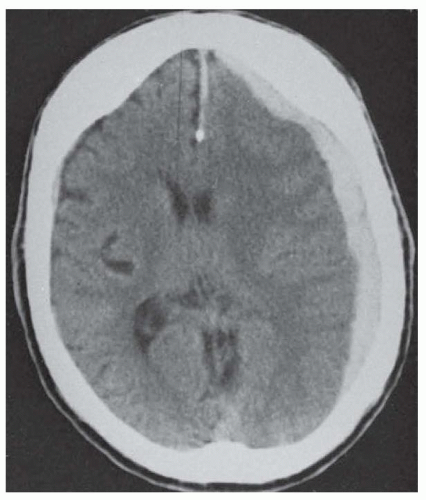
FIGURE 46.3 Traumatic intracerebral hemorrhage, frontal lobe. Axial noncontrast computed tomography demonstrates left frontal lobe density (hemorrhage), surrounding lucency (edema), and mass effect (sulcal and ventricular effacement). (Courtesy of Drs. S. K. Hilal and J. A. Bello.)
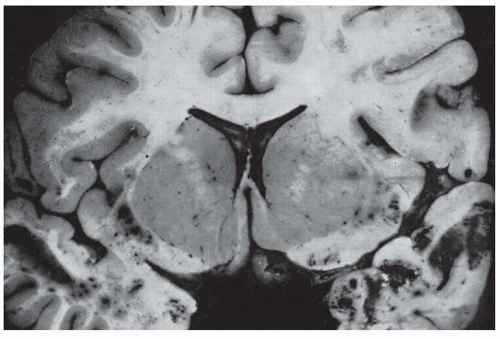
FIGURE 46.4 Pathologic specimen demonstrating traumatic contusions in the temporal lobes.
If there is no DAI, brain swelling, or secondary hemorrhage, recovery from one or more small contusions may be excellent. Healed contusions are often found at autopsy of people with no clinical evidence of permanent brain damage. Large, parenchymal hematomas with mass effect may require surgical evacuation.
Contusions are often managed conservatively unless they lead to significant symptomatic mass effect because they often consist of hemorrhagic or ecchymotic (but potentially viable) brain tissue.
SUBDURAL HEMATOMA
Subdural hematomas usually arise from a venous source, with blood filling the potential space between the dural and arachnoid membranes. In most cases, the bleeding is caused by movements of the brain within the skull that leads to stretching and tearing of “bridging” veins that drain from the surface of the brain to the dural sinuses.
Most subdural hematomas are located over the lateral cerebral convexities, but subdural blood may also collect along the medial surface of the hemisphere, between the tentorium and occipital lobe, between the temporal lobe and the base of the skull, or in the posterior fossa. CT usually reveals a high-density, crescentic collection across the entire hemispheric convexity (Fig. 46.5).
Elderly or alcoholic patients with cerebral atrophy are particularly prone to subdural bleeding; in these patients, large hematomas may result from trivial impact or even from pure acceleration-deceleration injuries, such as whiplash. Coagulopathy, including the use of oral anticoagulants, is another important risk factor for subdural hematoma and is associated with increased mortality.
Acute subdural hematomas, by definition, are symptomatic within 72 hours of injury, but most patients have neurologic symptoms from the moment of impact. They may occur after any type of head injury but seem to be less common after vehicular trauma and relatively more common after falls or assaults. Half of all patients with an acute subdural hematoma lose consciousness at the time of injury; 25% are in coma when they arrive at the hospital, and half of those who awaken lose consciousness for a second time after a “lucid interval” of minutes to hours as the subdural hematoma grows in size. Hemiparesis and pupillary abnormalities are the most common focal neurologic signs, each occurring in one-half to two-thirds of patients. The usual picture is ipsilateral pupillary dilation and contralateral hemiparesis. However, so-called false localizing signs are common with acute subdural hematoma because uncal herniation may lead to compression of the contralateral cerebral peduncle or third cranial nerve against the tentorial edge (Kernohan notch).
Chronic subdural hematomas become symptomatic after 21 days. They are more likely to occur in patients after age 50 years. In 25% to 50% of cases, there is no recognized episode of head injury. Risk factors for chronic subdural hematomas include cerebral atrophy, alcoholism, bleeding disorders or use of anticoagulant medication, and overdrainage of a ventriculoperitoneal shunt.
FIGURE 46.5 Acute subdural hematoma. Noncontrast axial CT demonstrates a hyperdense, crescent-shaped, extraaxial collection showing mass effect (sulcal and ventricular effacement) and midline shift from left to right. (Courtesy of Drs. J. A. Bello and S. K. Hilal.)
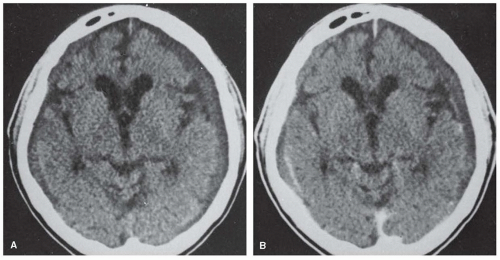
FIGURE 46.6 Bilateral chronic subdural hematoma. A: Noncontrast axial CT shows bilateral isodense extra-axial collections, larger on the left. B: These are better demonstrated on the postcontrast scan, in which enhancing membranes, typical of the subacute phase, may be seen. (Courtesy of Drs. J. A. Bello and S. K. Hilal.)
In many cases of chronic subdural hematoma, bleeding results from trivial trauma, and symptoms are minimal because the brain accommodates the gradual buildup of mass effect. After 1 week, fibroblasts on the inner surface of the dura form a thick outer membrane; after 2 weeks, a thin inner membrane develops, resulting in encapsulation of the clot, which eventually liquefies into a hygroma. Enlargement of the hematoma may then result from recurrent bleeding (acute-on-chronic subdural hematoma) or because of osmotic effects related to a high-protein content of the fluid. Symptoms may be restricted to altered mental status, a syndrome sometimes mistaken for dementia. CT typically shows an isodense or hypodense, crescent-shaped mass that deforms the surface of the brain, and the membranes may enhance with intravenous (IV) contrast (Fig. 46.6).
Symptomatic acute and chronic subdural hematomas with significant mass effect should be evacuated. Surgical evacuation of the thick, clotted blood that constitutes an acute subdural hematoma usually requires a large-window craniotomy. Outcome after surgical evacuation depends primarily on the severity of the initial deficit and the interval from injury to surgery. Liquefied chronic subdural hematomas are usually evacuated with drainage of the collections via a series of burr holes. Reoperations for acute and chronic subdural hematomas are required in about 15% of cases. Steroids have no role in the conservative management of smaller, minimally symptomatic, subdural hematomas.
EPIDURAL HEMATOMA
Epidural hematoma is a rare complication of head injury. It occurs in less than 1% of all cases but is found in 5% to 15% of autopsy series, attesting to the potential seriousness of this complication.
Bleeding into the epidural space is generally caused by a tear in the wall of one of the meningeal arteries, usually the middle meningeal artery, but in 15% of patients, the bleeding arises from a dural sinus. Seventy-five percent of patients are associated with a skull fracture. The dura is separated from the skull by the extravasated blood, and the size of the clot increases until the ruptured vessel is compressed or occluded by the hematoma.
Most epidural hematomas are located over the convexity of the hemisphere in the middle cranial fossa, but occasionally, hemorrhages may be confined to the anterior fossa, possibly as a result of tearing of anterior meningeal arteries. Extradural hemorrhage in the posterior fossa may occur when the torcular herophili is torn. In most cases, the hematoma is ipsilateral to the site of impact.
Epidural hematoma is primarily a problem of young adults; it is rarely seen in the elderly because the dura becomes increasingly adherent to the skull with advanced age. The clinical course, in one-third of patients, proceeds from an immediate loss of consciousness caused by concussion to a lucid interval and then to a relapse into coma, with hemiplegia as the epidural hematoma expands. The ipsilateral pupil loses reactivity to light because the third cranial nerve is stretched as the midbrain is displaced contralaterally. Later, it becomes fixed and dilated as the third nerve is compressed by the hippocampal gyrus as it herniates over the free edge of the tentorium.
As with acute subdural hematomas, false localizing signs may occur. The presence of cerebellar signs, nuchal rigidity, and drowsiness, together with a fracture of the occipital bone, should prompt suspicion of a clot in the posterior fossa.
Epidural blood takes on a bulging convex pattern on CT (Fig. 46.7) because the collection is limited by firm attachments from the dura to the cranial sutures. Progression to herniation and death may occur rapidly because the bleeding is arterial. The mortality rate approaches 100% in untreated patients and ranges from 5% to 30% in treated patients. As the interval between injury and surgical intervention decreases, survival improves. If there is little coexisting brain damage, functional recovery may be excellent.
TRAUMATIC SUBARACHNOID HEMORRHAGE
Some extravasation of blood into the subarachnoid spaces is to be expected in any patient with head injury. In most cases, subarachnoid blood is detected only by CSF examination and is of little clinical importance. With more serious injuries, when larger vessels traversing the subarachnoid space are torn, focal or diffuse subarachnoid hemorrhage may be detected by CT. In most cases, traumatic subarachnoid hemorrhage is distributed over the convexities. By contrast, spontaneous aneurysmal rupture results in bleeding into the basal cisterns. Although the presence of a large amount of subarachnoid blood is a poor prognostic sign, delayed complications of aneurysmal subarachnoid hemorrhage, such as hydrocephalus and ischemia from vasospasm, are unusual after traumatic subarachnoid hemorrhage.
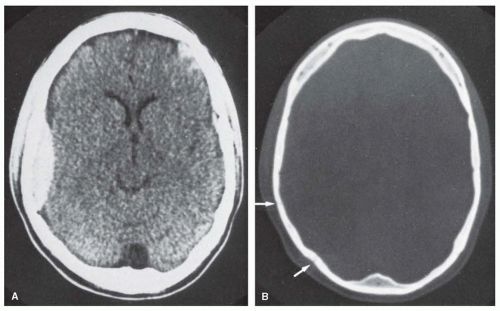
FIGURE 46.7 A: Epidural hematoma is evident on CT. B: CT with bone windows shows two adjacent fractures (arrows); the anterior fracture is at the site of the groove for the middle meningeal artery.
INITIAL ASSESSMENT AND STABILIZATION
On admission to the emergency room, resuscitation measures, history taking, and examination should begin simultaneously. The immediate goals of management are to assess and stabilize the airway, breathing, circulation, and disability (ABCD). The immediate goals of the initial neurologic assessment are to (1) perform a rapid screening neurologic examination; (2) classify the severity of the head injury as low, moderate, or high risk; (3) stabilize and rule out a fracture of the cervical spine; (4) begin empiric treatment for increased intracranial pressure (ICP) if it is suspected; and (5) perform an emergency CT scan of the head and neck to rule out bony fractures or intracranial bleeding. Careful screening at this time is also required to identify significant extracranial injuries.
CARDIOPULMONARY RESUSCITATION
Hypoxia and hypotension have a devastating effect on head-injured patients. If the patient is hypoxic (arterial oxygen saturation level <90%), in respiratory distress, or comatose and unable to protect his or her airway, endotracheal intubation should be performed urgently to be certain that the spine is immobilized during the procedure. Two doses of peri-intubation cefuroxime (1.5 g) may reduce the risk of subsequent pneumonia. Minute ventilation should initially be set to maintain a tidal volume of 6 mL/kg and rate of 8 to 12 breaths per minute, with the goal of maintaining the PCO2 between 30 and 40 mm Hg. The fraction of inspired oxygen can be quickly reduced from 100% to 40% as long as oxygen saturation levels are above 95%. Prophylactic aggressive hyperventilation (PCO2 <25 mm Hg) during the acute stage of injury may cause excessive vasoconstriction and aggravation of ischemic injury and is contraindicated.
Hypotension (systolic blood pressure [BP] <90 mm Hg) should be corrected with large-volume IV infusions of isotonic fluids such as normal saline or lactated Ringer solution (10 to 40 mL/kg) and blood transfusions or vasopressors as needed. Systolic BP during the stabilization phase should be maintained above 90 mm Hg to ensure adequate cerebral blood flow. If the patient is hypotensive, bleeding into the abdomen, thorax, retroperitoneal space, or tissues surrounding a long-bone fracture should be excluded by CT. Hypotension may also reflect spinal shock related to a coexisting spinal cord injury (see Chapter 47). Hypertension associated with wide pulse pressure and bradycardia (Cushing reflex) may reflect increased ICP or focal brain stem injury.
INITIAL NEUROLOGIC ASSESSMENT AND STABILIZATION
A baseline neurologic evaluation should be performed immediately while airway, respiration, and circulation are assessed. Injuries may be ranked as low, moderate, or high risk according to risk factors and a rapid initial neurologic assessment (Table 46.2). The skull should be palpated for fractures, hematomas, and lacerations. A step-off or palpable bony shelf is presumed to be a depressed skull fracture. A hard neck collar should be in place for all patients with any history of concussion, whiplash, or trauma above the level of the clavicles.
The Glasgow Coma Scale (GCS; Table 46.3) is based on eye opening and the patient’s best verbal and motor responses; these three individual scores should be recorded separately. The GCS is widely used as a semiquantitative clinical measure of the severity of brain injury; it also provides a guide to prognosis (Table 46.4). Patients who are comatose (GCS score ≤8), or who show clinical signs of herniation, require emergency interventions to reduce ICP, including 30 degrees of head elevation, hyperventilation to a target arterial PCO2 of 30 mm Hg, and 20% mannitol solution at a dose of 0.5 to 1.0 g/kg via rapid IV infusion (Table 46.5).
TABLE 46.2 Risk Stratification of Patients with Head Injury
Risk Category
Characteristics
Mild
Normal neurologic examination
No concussion
No drug or alcohol intoxication
May complain of headache and dizziness
May have scalp abrasion, laceration, or hematoma
Absence of moderate or severe injury criteria
Moderate
Glasgow Coma Scale score of 9-14 (confused, lethargic, stuporous)
Concussion
Posttraumatic amnesia
Vomiting
Seizure
Signs of possible basilar or depressed skull fracture of serious facial injury
Alcohol or drug intoxication
Unreliable or no history of injury
Age younger than 2, older than 65
Severe
Glasgow Coma Scale score of 3-8 (comatose)
Progressive decline in level of consciousness (“talked and deteriorated”)
Focal neurologic signs
Penetrating skull injury or palpable depressed skull fracture
Adapted from Masters SJ, McClean PM, Arcarese JS, et al. Skull x-ray examinations after head trauma. Recommendations by a multidisciplinary panel and validation study. N Engl J Med. 1987;316(2):84-91.
HISTORY
The circumstances of the accident and the clinical condition of the patient before admission to the emergency room should be ascertained from records of the emergency medical services, the patient (if possible), and eyewitnesses. The force and location of head impact should be determined as precisely as possible. Specific inquiry should be made about concussion; because patients are amnesic during the concussion, only an eyewitness may accurately gauge the duration of loss of consciousness.
Patients who have “talked and deteriorated” should be assumed to have an expanding intracranial hematoma until proven otherwise. Reports of headache, nausea, vomiting, confusion, or seizure activity must be noted. A medical history, including medications and drug and alcohol use, should be obtained. Recent drug and alcohol use occurs in many trauma patients.