TABLE 53.1 Proposed Types of Vascular Dementia Based on Localization and Pathophysiologic Mechanism | ||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
and 5% per year become demented thereafter. On a clinical basis, vascular dementia has been long considered as the second (after Alzheimer disease) or even the third (after Alzheimer and dementia with Lewy bodies) most frequent cause of dementia. Considering pathologic series data and related clinical-pathologic correlations makes the issue quite more complex.
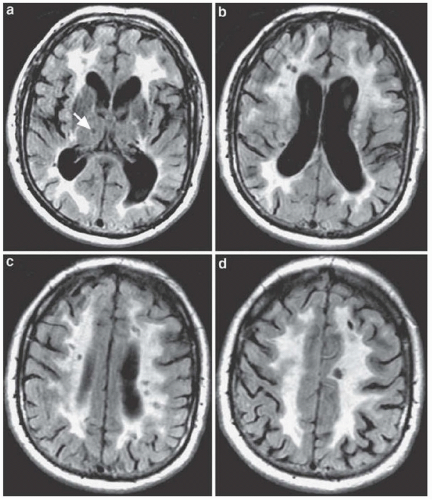 FIGURE 53.1 Binswanger disease in an 85-year-old man with dementia. A-D: Axial fluid-attenuated inversion recovery magnetic resonance images show extensive symmetric hyperintensity involving periventricular and lobar white matter. These lesions have a rather sharp outer border and show sparing of the U-fibers. This diffuse involvement was considered more than 25% of the total white matter. There are also a lacunar right thalamic infarct (arrow), several bilateral hypointense lesions within the periventricular hyperintensity representing lacunar infarcts and an important global cerebral atrophy. (From Guermazi A, Miaux Y, Rovira-Cañellas A, et al. Neuroradiological findings in vascular dementia. Neuroradiology. 2007;49[1]:1-22.) |
standard neuropathologic examinations performed on autopsy, suggesting limited sensitivity of neuropathology for detection of cerebrovascular damage.
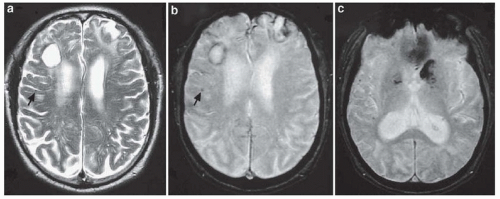 FIGURE 53.2 Amyloid angiopathy in a 66-year-old man with dementia. A: Axial spin-echo T2-weighted MR image shows bilateral large frontal hemorrhages surrounded by a rim of hypointensity due to hemosiderin deposition. There is also another right frontal punctate hypointense lesion (arrows), best seen on B, the axial gradient echo T2-weighted MR image. C: Axial gradient echo T2-weighted MR image caudal to B shows additional hypointensities bilaterally in the basal ganglia and the right parietal lobe (From Guermazi A, Miaux Y, Rovira-Cañellas A, et al. Neuroradiological findings in vascular dementia. Neuroradiology. 2007;49[1]:1-22.) |
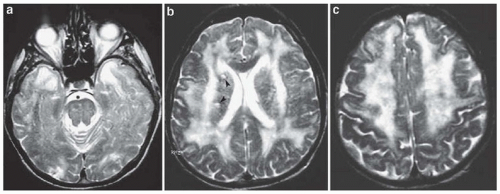 FIGURE 53.3 CADASIL in a 57-year-old man with cognitive impairment. A: Axial spin-echo T2-weighted MR images show an extensive white matter abnormalities with characteristic symmetric involvement of the anterior part of the temporal lobes and (B) external and extreme capsules without involvement of the internal capsules. They also show (C) extensive white matter changes in the centrum ovale, extending toward the cortex in some places. There are also two small lacunar infarcts in the right basal ganglia (arrowheads). (From Guermazi A, Miaux Y, Rovira-Cañellas A, et al. Neuroradiological findings in vascular dementia. Neuroradiology. 2007;49[1]:1-22.)
Related posts:Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

|
