“The single biggest threat to man’s continued dominance on the planet is a virus.”
— Joshua Lederberg, Nobel Prize winner
INTRODUCTION
Viral infections of the central nervous system (CNS) are a diverse group of diseases that have plagued mankind for centuries. Infections can occur in the spinal cord (myelitis), cerebrum (encephalitis), meninges (meningitis), brain stem (rhombencephalitis), or any of these in combination. Additionally, viral infections at disparate sites may damage the CNS indirectly through a misguided immune response. This chapter highlights the common causes of CNS viral infections (aside from HIV, which is discussed in a separate chapter), discusses the clinical manifestations and the methods of detection, and when applicable, reviews treatment options.
Viruses invade humans by a variety of mechanisms. This can include skin penetration, infection of mucosal membranes, such as in respiratory or gastrointestinal epithelium, or by direct inoculation into the bloodstream. After primary inoculation, neurotropic viruses gain entry into the CNS by one of a number of mechanisms.
Experiments with several viral strains show that replication occurring in tissue, such as skeletal muscle or skin, allows access to peripheral nerve endings. Some neurotropic viruses are able to infect nerves and then spread by retrograde transport to the sensory ganglia. Characteristic of this is the herpes simplex virus, which replicates in the skin and infects adjacent sensory nerve endings. The virus is then able to tether its capsid onto the host’s transport complex, travel toward the dorsal root ganglia, and establish latency.
On the other hand, infection within the bloodstream is dependent on the site of inoculation and ability to infect endothelial cells or cell populations within plasma (e.g., HIV infection of T lymphocytes). Once in the blood, a virus must cross the blood-brain barrier (BBB) to spread into brain parenchyma. In cases like HIV, when infected inflammatory cells, such as lymphocytes or macrophage mononuclear cells cross the BBB, the virus gains entry in a process termed the Trojan horse. In other cases, high viremic loads lead to passive transport into the brain or spinal cord. Individual viruses can use multiple mechanisms of viral CNS entry, and in fact, many viruses are able to spread to the CNS using both neural and hematogenous pathways as will be discussed with poliovirus and varicella-zoster virus (VZV).
The widespread availability of viral nucleic acid amplification has revolutionized diagnostics in CNS viral infections and reduced the need to perform open brain biopsies. The polymerase chain reaction (PCR) technique is ideally suited for organisms that are difficult to culture and can retain its sensitivity even after small doses of antiviral therapies. However, this technique relies on a viral load high enough for detection by PCR, a factor not always present in cerebrospinal fluid (CSF), leading to false negatives. False negatives also occur when heme breakdown from a bloody lumbar puncture interferes with nucleic acid detection. Falsepositive CSF PCR results occur with viruses that associate themselves with peripheral blood cells and enter the CNS during an inflammatory process but are themselves not the source of the CNS disorder. This phenomenon occurs with Epstein-Barr virus (EBV), as peripheral blood mononuclear cells are latently infected. EBV’s relevance as a pathologic agent in the CSF can be unclear and is discussed further in this chapter.
Additional diagnostic methods for CNS viral infections include detection of virus-specific immunoglobulin (Ig) M that relies on the host’s ability to mount an immunologic response to the infecting agent. The detection of virus-specific antibodies requires a competent immune system and sufficient time to develop antibodies. Interpretation of antibody levels can be confusing, as some serum antibodies last for months or even years after infection that is often asymptomatic, as seen in West Nile virus where IgM-specific antibodies can persist for months and is not reflective of acute infection. Occasionally, antibody cross-reactivity can also lead to false-positive detection. In contrast to serum antibodies, the presence of virus-specific IgM antibodies in CSF is indicative of intrathecal synthesis and diagnostic of neuroinvasive disease.
Serum virus-specific IgG can be helpful when a corresponding rise in titer between acute and convalescent phases occurs. One limitation here is in the setting of postinfectious complications, where antibody detection in the acute phase was not pursued. Isolated IgG detection, especially in infections that are common and usually asymptomatic, is of limited use.
Antiviral agents are few in number, and treatment in many cases of CNS viral infections remains supportive. Herpes simplex virus, VZV, cytomegalovirus, HIV, and influenza have targeted therapies with varying efficacy. The lack of options in many cases leads physicians to focus on managing the complications of these diseases, often including use of anti-inflammatory agents, such as corticosteroids, to suppress immune-mediated injury. As seen in almost every aspect of medicine, prevention is the best approach to combatting viral diseases and requires comprehensive vaccination programs, mosquito repellents, appropriate protective gear, animal surveillance programs, and education.
PICORNAVIRUS
Picornaviruses are some of the oldest and most diversified viruses to cause human disease. The picornavirus family has four primary groups resulting in human pathogenesis: enteroviruses (e.g., polioviruses, coxsackieviruses, and echoviruses), rhinoviruses (RV), hepatoviruses (e.g., hepatitis A), and parechoviruses. These viruses are nonenveloped, single-stranded RNA viruses. It is estimated that the majority of viral meningitis cases globally are caused by picornaviruses, specifically enteroviruses, as are most cases of acute flaccid paralysis.
ENTEROVIRUSES
Poliomyelitis
Poliomyelitis is a disease that plagued the world in the late 19th and early 20th century, as widespread epidemics resulted in paralysis or death. The name poliomyelitis is derived from two Greek words, polios (“gray”) and meylon (“marrow” or “spinal cord”). The control of polio following the development of both the inactivated polio vaccine (IPV) and live-attenuated oral vaccines (OPV) is a remarkable achievement in science. In the United States, the last case of naturally occurring polio was in 1979. There continues to be endemic areas, namely in Afghanistan, Nigeria, and Pakistan, with additional occasional outbreaks elsewhere. The worldwide eradication of polio is the goal of the World Health Organization (WHO) and many countries, as well as nonprofit organizations.
PATHOBIOLOGY
Poliomyelitis virus is an enterovirus whose main route of human infectivity is via the gastrointestinal tract. There are three serotypes (types 1, 2, and 3), with all serotypes being neurotropic. Poliovirus type 1 is the most frequently encountered in human infections around the world. Although the disease occurs in all age groups, it is rarely seen before 6 months of age. Infections are spread via the fecal-oral route and are highly influenced by hygiene standards. The virus replicates initially in the gastrointestinal tract’s lymphatic system (Peyer patches), followed by viremia and immune activation. How the virus gains access to the nervous system remains uncertain. One hypothesis is the poliomyelitis virus, which is able to replicate in skeletal muscles, can spread into peripheral motor axons, and access anterior horn cells of the spinal cord via retrograde transport. This hypothesis has been tested in mouse models with expression of transgenic poliomyelitis virus receptor. A second hypothesis is by direct spread from the blood due to a breakdown in the BBB. These mechanisms for CNS entry are not mutually exclusive.
CLINICAL MANIFESTATIONS
Although CNS complication is the most feared outcome of polio infection, it is a not a common occurrence when evaluating poliomyelitis infections as a whole. Nearly 90% of infections are asymptomatic and recognized only by isolation of the virus from the oropharynx or in feces. Approximately 4% to 8% of those infected will have a minor, self-limited illness similar to other enteroviral infections with headache, anorexia, abdominal pain, and a sore throat. These cases are typically identified during epidemics. In 1% to 2% of infected individuals, there are the more severe clinical manifestations of fever, headache, and evidence of meningismus. Frank paralysis occurs in only 0.1% of all poliovirus infections, and the clinical course can be divided into two phases. A prodromal phase of sore throat, fever, and symptoms suggestive of upper respiratory infection is most common in young patients. Mild abdominal upset and meningeal irritation are more common in adults. There is a short recovery period for 2 to 3 days before an abrupt onset of fever, chills, myalgias, headache, and symptoms consistent with meningitis. Paresthesias and muscle fasciculations can precede muscle weakness and paralysis. When paralysis occurs, it is typically asymmetric, and the lower extremities are more commonly involved than the upper extremities. When quadriplegia occurs, it is more frequently seen in adults than infants. Paralysis of the diaphragm and intercostal muscles in spinal poliomyelitis occurs more often in young adults than in the extreme age groups. Bulbar paralysis is due to weakness of muscle groups innervated by cranial nerves, and in polio, the glossopharyngeal and vagus nerves are most commonly affected, followed by the oculomotor nerve. Older adults are more likely to have medullary involvement, and these patients are at high risk for aspiration and need for mechanical ventilation.
DIAGNOSIS
The diagnosis of paralytic polio is clinically suspected with the development of asymmetric acute flaccid paralysis following a febrile illness. It is more likely to be suspected in those who are unvaccinated coming from endemic countries or those with immunodeficiencies. Other viruses to consider in the differential are other enteroviruses, especially enterovirus 71, and arboviral infections, such as West Nile virus (discussed later in the chapter).
CSF pleocytosis is evident as early as meningeal symptoms are present, with an initial polymorphonuclear profile that eventually shifts to a lymphocytic predominance. An increased protein concentration is most prominently seen if there is severe paralysis. These abnormalities are not distinguishable from other viral causes of aseptic meningitis and thus, identification of the poliomyelitis virus is necessary to confirm the diagnosis. Isolation of poliomyelitis virus by CSF culture is challenging and is not typically performed. Polio is more easily isolated from oral secretions and feces, and with rapid identification of polioviruses by genomic amplification using PCR, clinicians can distinguish poliomyelitis viral infections from other enteroviruses or other infectious causes.
TREATMENT
There are no antiviral drugs for treatment of poliomyelitis, and symptom management is the primary focus. Respiratory muscle paralysis or cases of bulbar poliomyelitis frequently require mechanical ventilation and aggressive management of secretions. Bowel function also requires special attention in spinal poliomyelitis. Long-term management of physical and psychiatric sequelae obliges a comprehensive team of both physical and occupational therapy along with orthopedic services and psychiatry.
The inactivated and oral poliomyelitis vaccinations have been used effectively for controlling paralytic poliomyelitis but differ in terms of asymptomatic viral shedding and risk of contracting vaccine-related disease. IPV is an injectable preparation containing antigen units for all three polio serotypes. In the United States, the IPV is the only version administered and is typically given with other childhood vaccines at 2, 4, 6 to 18 months, and 4 to 6 years. Children develop little to no secretory antibody response to the IPV. If exposed to live polioviruses, these children are more likely to have asymptomatic infections but still shed virus in their feces, exposing nonimmunized contacts. Most oral poliomyelitis vaccine (OPV) preparations also immunize against all three serotypes. The prevalence of poliomyelitis-specific antibody to all three serotypes following three doses of OPV is approximately 96%. Nonimmune OPV recipients will shed vaccine viruses in feces and the oropharynx that can be spread to nonimmunized children. This aspect can be advantageous in poorly vaccinated communities, as children can develop OPV-specific antibodies despite not having received the vaccine. A rare event is the development of vaccine-associated paralytic poliomyelitis, an occurrence in 1 per 2.6 million vaccine doses and is only associated with OPV. The WHO still recommends the use of the trivalent OPV in underdeveloped nations because of cost, ease of administration, and greater secretory immunity in the gastrointestinal tract.
OUTCOME
The prognosis of paralytic poliomyelitis depends on age (infants and children are more likely to recover) and severity of paralysis (i.e., partial vs. complete paralysis). Permanent weakness from polio paralytic infections occurs in approximately two-thirds of patients. Complete recovery is unlikely in cases with severe acute flaccid paralysis or in those requiring mechanical ventilation. Increased mortality is typically seen in those with polio encephalitis, bulbar involvement due to glossopharyngeal and/or vagus nerve impairment, and/or respiratory muscle paralysis.
Following the epidemics in the early 20th century, some individuals with partial or full recovery from paralytic polio experienced a new onset of neuromuscular weakness, pain, and fatigue. In such cases, muscle weakness and atrophy were identified in muscles that had been previously affected. These symptoms have been collectively called the postpolio syndrome and, in those with slowly progressive weakness, atrophy, and fasciculations, termed postpolio progressive muscular atrophy (PPMA; discussed separately).
Enteroviruses 70 and 71
Acute hemorrhagic conjunctivitis was first recognized in 1970 and is the result of either enterovirus 70 or an antigenic variant of coxsackievirus A24. The disease is characterized by the rapid onset of painful conjunctivitis and subconjunctival hemorrhage. Complete recovery is typically seen within 1 to 2 weeks. Epidemics predominantly occur in tropical and subtropical regions lasting several months and will affect large populations.
Neurologic complications of acute hemorrhagic conjunctivitis primarily include an asymmetric acute flaccid paralysis. Those affected appear clinically similar to those with spinal poliomyelitis except for the preceding association with acute hemorrhagic conjunctivitis. Prodromal symptoms for acute hemorrhagic conjunctivitis-associated paralysis include fever and malaise then an acute, severe radicular pain. This is followed by flaccid, asymmetric weakness of the legs with proximal muscles (e.g., quadriceps muscle) more affected. Reflexes are diminished or absent. Permanent paralysis or residual weakness is present in over half the cases. The virus is difficult to isolate in the CSF by PCR when neurologic symptoms arise, but high titers of virus-specific antibodies are typically detectable in the CSF in those with paralysis.
Enterovirus 71 has been the etiologic agent responsible for several encephalitis epidemics throughout the world, resulting in substantial mortality and morbidity. The largest enterovirus 71 epidemic occurred in Taiwan in 1988, resulting in 1.5 million people affected, of which 405 children developed serious neurologic complications with 78 deaths. Every 2 to 3 years, large enterovirus 71 outbreaks occur around the Asia-Pacific rim, affecting thousands. As such, enterovirus 71 is now recognized as an emerging neurotropic virus. Enterovirus 71 can cause hand-foot-and-mouth disease as well as upper respiratory infections and gastroenteritis. In those affected neurologically, manifestations include myoclonic jerks, tremors, ataxia, cranial nerve palsy, meningitis, and meningoencephalitis. Polio-like flaccid paralysis occurs in about 10% of patients. Fulminant neurogenic pulmonary edema and apnea from rhombencephalitis occurred in epidemics affecting children in Taiwan and Malaysia, and these disease manifestations are the primary cause of death in enterovirus 71-infected individuals. Most of the patients had magnetic resonance imaging (MRI) T2-weighted high-intensity lesions in the brain stem. Diagnosis may be made by virus isolation from throat, feces, or vesicles; by antibody studies; and CSF reverse transcriptase polymerase chain reaction (RT-PCR).
COXSACKIEVIRUS AND ECHOVIRUSES
Neurologic manifestations of human viral infections caused by group A and group B coxsackieviruses and echoviruses primarily are meningitides. Historically, group B coxsackieviruses and echoviruses are the most frequently implicated serotypes in meningitis; exceptions include when a single serotype causes a widespread outbreak. For example, coxsackievirus A9 was responsible for most cases in an outbreak in the Gansu Province, China in 2005 and Alberta, Canada in 2010.
The symptoms and signs of meningeal involvement of coxsackieviruses and echoviruses are similar to other viruses that cause meningitis. The severity of disease varies, with the extremes of life having the more severe meningitis. Headache is frequent, and if meningismus is present, it can vary in severity and typically begins 24 to 48 hours following onset of symptoms. In infants, the dominant symptoms are fever and irritability, with less than 10% having evidence of meningeal irritation. Frequently, there is a prodromal or associated upper respiratory tract infection or symptoms. Acute CNS complications include febrile seizures, elevated intracranial pressure, and coma. When considering alternate diagnoses for enterovirus meningitis, bacterial meningitis needs to be considered and should be treated empirically with broad-spectrum antibiotics. Arboviruses, acute HIV, herpesviruses, Lyme borreliosis, leptospirosis, and lymphocytic choriomeningitis virus are other infectious etiologies in the differential.
CSF analysis typically demonstrates clear fluid with normal to mildly elevated pressure. There is a mild to moderate pleocytosis that ranges from 10 to 500/mm3 and rarely exceeds 1,000/mm3. Initial differential cell counts demonstrate a high percentage of neutrophils but an eventual shift to a lymphocytic predominance. The CSF glucose concentration is generally normal and protein concentrations are normal to slightly elevated. PCR is the primary means of virus detection with greater than 95% sensitivity and specificity. Viral cultures are infrequently used, as they are insensitive and can take days for results to return.
Treatment is largely symptom management. Containment during outbreaks is critical, with good hygiene practices and protective equipment for high-risk groups. The broad-spectrum antipicornaviral agent pleconaril is an orally administered inhibitor of enterovirus replication. There have been two placebo-controlled clinical trials that showed a shortened course of illness compared to placebo, but the benefit was modest. The drug has not been approved for use in the United States.
Although encephalitis is not commonly caused by coxsackievirus or echovirus (with the exception of enterovirus 71), it can occur in immunocompromised patients. The severity of encephalitis is variable, with seizures, hemichorea, and acute cerebellar ataxia being described. In patients with agammaglobulinemia, hematopoietic transplantation, or B-cell depletion with immunotherapy agents, enterovirus can cause a chronic, severe, and fatal meningitis and encephalitis. In such cases, enterovirus can be recovered in the CSF by PCR at different time points throughout the disease course. Intravenous immunoglobulin (IVIg) and pleconaril have been used with some success.
Sporadic cases of acute flaccid paralysis have been seen with coxsackieviruses and are typically less severe than in poliovirusassociated disease. For example, in an 11-year program monitoring of acute flaccid paralysis in the Slovak Republic as part of the WHO strategy for polio eradication, coxsackievirus B and echoviruses were the most common etiologies for acute flaccid paralysis in the post-polio vaccine era. These viruses are also reported etiologies for oculomotor palsies, Guillain-Barré syndrome (GBS), opsoclonus-myoclonus, and transverse myelitis.
ARBOVIRUSES
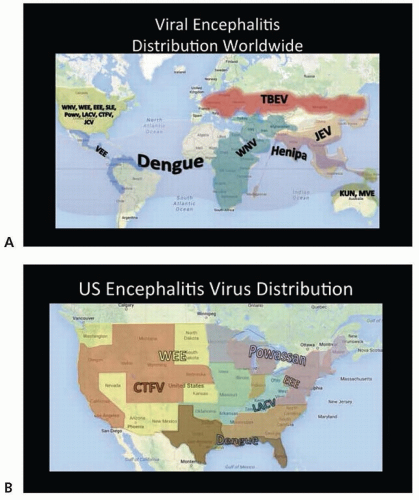
Arboviruses comprise a group of viruses from four genera that all have in common transmission to humans via arthropods: alphaviruses, flaviviruses, bunyaviruses, and reoviruses. Human infection due to arboviruses follows patterns of vector activity. That is to say that seasons and years when the insects are most abundant logically see higher rates of infections. Most arboviruses have vertebrate reservoirs, such as birds or small mammals, and are transmitted by mosquitoes or ticks. Continuation of the life cycle relies on a constant interaction between hosts (e.g., birds, mammals) and vectors (e.g., ticks, mosquitoes). Animals that act as hosts maintain high enough levels of viremia and are able to retransmit infections back to arthropods when bitten. However, humans and horses are “dead-end” hosts, as they are not able to sustain elevated levels of viremia without succumbing to disease. Endemicity varies widely, as do outcomes. Figure 66.1 demonstrates highly endemic areas for many encephalitis-associated viruses.
Arboviruses are important causes of encephalitis worldwide, and neuroinvasion is usually coupled with an intense inflammatory reaction and/or edema, the effects of which can be devastating. Alternatively, neurologic disease can occur as a parainfectious inflammatory disorder in the setting of systemic disease without specific evidence of nervous system infection per se. Fortunately, for the most part, exposure leads to asymptomatic seroconversion or a mild self-limited illness; typically, only a fraction progress to severe neurologic disease and/or death.
FIGURE 66.1 A: Global distribution of viral etiologies of encephalitis. Herpesviruses and rabies are excluded, as these are all ubiquitous around the globe. United States and Canada are endemic to multiple viruses but most vary by region. B: Distribution of nonherpes, non-WNV, and non-SLE viral encephalitis viruses in the United States. WNV has been reported from all continental states, and St. Louis has only not been seen in New England.
Acute arboviral infections are diagnosed typically by serum and/or CSF antibody detection via enzyme-linked immunosorbent assay (ELISA) for virus-specific IgM antibodies. Given the high prevalence of asymptomatic infection and potential for persistence of IgM in serum, antibody detection must be confirmed with a fourfold titer increase in IgG between the acute and convalescent phase (4 weeks post the acute phase). In general, though, the presence of CSF virus-specific IgM antibodies is indicative of intrathecal synthesis and is diagnostic for neuroinvasive disease. CSF RNA detection is highly specific for active infection, but its sensitivity in arboviral infections is not nearly as high as seen in herpes simplex DNA detection. CSF PCR can be especially helpful in immunocompromised people who are unable to mount or have a delayed antibody response. Culturing arboviruses is not routinely performed, as they are difficult to isolate due to low levels of viremia in humans. There are no specific antiviral therapies for the treatment of neuroinvasive arboviral infections and the focus remains on supportive care and exposure prevention.
FLAVIVIRUSES
Flaviviruses are positive-sense, single-stranded, enveloped viruses with icosahedral capsids. Many have the capability of neuroinvasion and severe damage throughout the neuraxis. Inflammatory reactions accompany infection. Table 66.1 outlines the most consistently described statistics for flaviviruses that cause neurologic disease.
Dengue
There are four serotypes of this flavivirus, and infection with one does not confer protection from infection with the others. Dengue is carried by the Aedes mosquito and can be acquired throughout Central and South America, Puerto Rico, Africa and the Middle East, Southeast Asia and the Pacific, and Australia (see Fig. 66.1A). The southern United States occasionally sees cases as well. Millions are infected each year. Vertical transmission is also known, as is spread through infected blood and organ donation.
PATHOBIOLOGY
As with other flaviviruses, inoculation proceeds to local immune cell infection and carriage to a lymph center, where replication occurs and viremia results. The virus makes its way to the CNS, although mechanisms of infection are not well understood. Virus is detected in the CNS, although it is not known if this occurs passively across an altered BBB or as an active infection. Vasogenic edema results, and a systemic inflammatory response can elicit immune-mediated damage of multiple organs and the neuraxis.
CLINICAL MANIFESTATIONS
After exposure and subsequent incubation of several days to just over a week, those who are symptomatic will experience fever, myalgias, and malaise most commonly, occasionally with a rash. Severe systemic disease can follow over a matter of days, characterized by thrombocytopenia, multifocal hemorrhage, shock, and death. Neurologic manifestations can accompany severe disease and range from encephalopathy to direct nervous system infection accompanied by an inflammatory response causing meningoencephalitis and/or myelitis to a parainfectious immune diseases such as GBS and acute disseminated encephalomyelitis (ADEM). Up to 50% of those who are symptomatic will develop neurologic complications. Risk factors for developing severe disease include young age, certain HLA genotypes, female gender, and superinfection with a second serotype. Serotypes 2 and 3 are associated more so with neuroinvasive disease than are the others.
TABLE 66.1 Nervous System Disease Caused by Flaviviruses
Virus
Endemic Locale
No. of Infections Annually
Systemic Symptomatic Disease (% of Infections)
Neurologic Disease (% Symptomatic Infections)
Neurologic Manifestations
Case Fatality Rate
Long-term Sequelae
Preventive Strategies
Japanese encephalitis virus
Southeast Asia, Japan, Pacific Islands
30,000-50,000
0.30
0.001-0.02
Encephalitis with brain stem and occasionally spinal cord involvement
25%
30%
Vector control, vaccine
West Nile virus
Africa, Middle East, Continental United States, Puerto Rico
Vector control, blood and organ donation restrictions
Dengue virus
Central and South America, Puerto Rico, Africa, Middle East, India, Southeast Asia, Pacific Islands, Northern Australia
50-400 million
0.5-1
4-50
Meningoencephalitis, ADEM, GBS, CNS hemorrhage
4%-5%
˜25%
Vector control
Murray Valley encephalitis virus
Northern Australia, New Guinea
Occurs in outbreaks
Outbreaks of 21-114 cases
0.1-0.7 of all infections
Meningoencephalitis
20%-40%
30%-50%
Vector control
Tick-borne encephalitis virus
Europe, Southern Russia, East Asia
˜35,000
2-33
25-30
Meningoencephalitis
1%-2% (Western Europe) 30%-40% (Eastern Russia)
35%-60%
Vector control, vaccine
Kunjin virus
Northern Australia, New Guinea
Occurs in outbreaks
Minority
Minority
Mild meningoencephalitis or encephalomyelitis
<1%
NA
Vector control
St. Louis encephalitis virus
Continental United States
˜1,000; higher in outbreaks
<1
>60
Meningoencephalitis
5%-15%
Up to 50%
Vector control
Powassan virus
Canada, Northern United States, Russia
NA; seroprevalence 0%-5% in endemic areas
Minority
NA; <50 cases reported 2001-2012 but incidence rising
Meningoencephalitis and/or encephalomyelitis
10%
50%
Vector control
ADEM, acute disseminated encephalomyelitis; GBS, Guillain-Barré syndrome; CNS, central nervous system; NA, not applicable.
DIAGNOSIS
Given the protean neurologic complications, there is no specific neuroimaging finding related to dengue, and computed tomography (CT) or MRI of the brain may be entirely normal. Similarly, CSF may be normal or only demonstrate elevated protein concentration; this appears to relate to the type of neurologic complication present. Opening pressures can also be elevated. If there is a pleocytosis, it is generally lymphocytic. If caught early, RNA can be detected from the blood and/or CSF; otherwise, antibody detection from blood and/or CSF demonstrating active or recent production is diagnostic. In endemic areas, a tourniquet test to assess capillary fragility can be performed at the bedside in the appropriate clinical context to make a presumptive diagnosis.
TREATMENT
No vaccine or specific therapies exist for dengue infection, although aggressive supportive treatment early on, with platelet transfusions, rehydration, and management of elevated intracranial pressure, may improve survival. Case fatality rate is 4% to 5%, although some 25% of survivors will suffer residual neurologic deficits (see Table 66.1).
Tick-Borne Encephalitis Virus
Tick-borne encephalitis virus is carried by the Ixodes tick. It is found across Europe and Asia and is responsible for thousands of infections each year (see Fig. 66.1A). Men are more commonly affected than women. Viral infection results in replication in lymphatic cells, vascular dispersion, and entry into brain parenchyma by means of brain microvascular endothelial cells. Viral presence in the brain incites an inflammatory reaction that precipitates widespread damage throughout the cerebrum, cerebellum, brain stem, and sometimes the spinal cord. After an incubation period of about a week, patients develop a fever that lasts several days and then progresses to headache, nausea, and occasionally meningismus. They can further develop encephalopathy and brain stem dysfunction several days later, and in the most severe cases, severe back pain and upper more so than lower extremity paresis can occur. Diagnosis is best made by demonstration of intrathecal tick-borne encephalitis virus-specific antibody production; serum antibodies can be useful in the patient who has never received vaccination. CSF usually shows a modest lymphocytic pleocytosis and elevated protein concentration, although in some cases, a polymorphonuclear pleocytosis has been demonstrated.
Treatment of tick-borne encephalitis virus is supportive. Mortality varies by location, at 1% to 2% for Western Europe but up to 40% for Eastern Russia (see Table 66.1). Long-term neuropsychiatric sequelae occur in more than half of the survivors. An effective vaccine exists, but for a variety of reasons, vaccination rates overall remain low.
Japanese Encephalitis Virus
Japanese encephalitis virus is transmitted by the Culex mosquito. It was first identified in Japan in 1871 but now includes much of Southeast Asia (see Fig. 66.1A). Like its sibling flaviviruses, initial replication is in lymphoid tissue followed by transient viremia that carries the virus to the brain; once inside the CNS, it imparts damage both by infection and reactive inflammation.
Most Japanese encephalitis virus infections are asymptomatic; about 1 in 300 is clinically apparent. Somewhere between 1 and 20 in 1,000 produce neuroinvasive disease. This translates, though, into some 50,000 cases of encephalitis a year, with a mortality rate of about 25%. Children and young adults are at highest risk.
In symptomatic cases, after an incubation period of a little over a week, fever sets in, along with chills, myalgias, and occasionally meningismus. In children, abdominal pain and nausea are common. Symptoms can quickly progress to limb weakness and extrapyramidal signs and subsequently to coma and death. Imaging and pathologic specimens show thalamic and cerebral peduncular involvement, but viral involvement is typically widespread throughout the brain and even into the spinal cord occasionally. CSF typically shows a lymphocytic pleocytosis of up to 1,000 cells/µL and a modestly increased protein concentration. Diagnosis is usually by antibody detection from CSF or by serologic increases between acute and convalescent phases; RNA isolation from CSF is diagnostic, as well. As with other flavivirus infections that are usually asymptomatic and/or have vaccines available, a single positive IgG in endemic areas may not indicate active disease.
Treatment is supportive, keeping in mind that death commonly is secondary to cerebral edema and increased intracranial pressure. Of those who survive, about 30% will have long-term deficits (see Table 66.1), again making prevention strategies key. These include vector control and vaccination; there is a highly effective vaccine for Japanese encephalitis virus, but vaccination campaigns are unfortunately currently lacking.
West Nile Virus and Kunjin Virus
West Nile virus was originally isolated in Africa but since introduction to New York in 1999 has been endemic in the United States (see Fig. 66.1A). Its vector is the Culex mosquito, although infected donated blood has been another mode of transmission. As of 2012, all 48 contiguous states in the United States had reported cases. Most cases of West Nile virus are asymptomatic and go unreported; there were an estimated 1.8 million infections in North America between 1999 and 2010. Hundreds to thousands of symptomatic cases are reported to the Centers for Disease Control and Prevention (CDC) each year. As such, seroprevalence of West Nile virus IgG in endemic areas is actually quite high. Of the symptomatic cases, the most common symptoms are fever and malaise. Less than 1% will go on to develop what is considered neuroinvasive disease: meningitis, encephalitis, or myeloradiculitis. Risk factors for developing neuroinvasive disease are age older than 50 years, immune suppression, homelessness, chronic renal disease, hepatitis C infection, and CCR5 mutations.
PATHOBIOLOGY
West Nile virus has an incubation period of 2 to 14 days, after which replication occurs in lymph tissue, followed by viremia and carriage to the CNS, where it infects neurons and anterior horn cells. How it does so remains elusive, as receptors have not been identified. Nor is it known how the virus crosses the BBB. As with many viral CNS diseases, though, its mechanism of neuronal injury and death is not only directly related to viral infection but also to the intense inflammatory reaction that imparts bystander damage to the delicate resident cells in the brain and spinal cord.
CLINICAL MANIFESTATIONS
West Nile virus neuroinvasive disease presentation depends on the part of the neuraxis that is involved. Fever, headache, meningismus, and encephalopathy herald meningoencephalitis, whereas radicular pain and flaccid asymmetric limb paralysis accompany anterior horn cell infection. New parkinsonism points to basal ganglia involvement.
DIAGNOSIS
Diagnosis can be made by detection of West Nile virus RNA in the CSF, although this is fleeting and insensitive after about 48 hours, or by CSF IgM or by a fourfold increase in antibody titers from acute to convalescent phase. CSF otherwise should demonstrate a lymphocytic pleocytosis with moderately elevated protein concentration and normal glucose concentration; however, neutrophilic predominance can also be seen. Although West Nile virus RNA can be detected in urine, use of this assay in acute disease is not standard. Neuroimaging may be normal or may demonstrate leptomeningeal enhancement; radicular enhancement; and/or T2 hyperintensities in the subcortical white matter, deep gray matter structures, and/or the spinal cord parenchyma.
TREATMENT
As with many viruses, West Nile virus is a monophasic illness for which there is no proven specific therapy other than supportive therapy. IVIg, West Nile virus-specific IgG, and ribavirin all have been not clearly beneficial, but corticosteroids are commonly used to modulate inflammation. Long-term sequelae are the rule for survivors of neuroinvasive disease, and about 10% die (see Table 66.1), making prevention of mosquito bites the most logical management strategy.
Kunjin is a subtype of West Nile virus isolated in northern Australia that primarily causes disease in horses; human disease has been reported and is similar to but much milder than West Nile virus neuroinvasive disease (see Fig. 66.1A). It can be transmitted to humans, also by the Culex mosquito, and occurs typically in small outbreaks (see Table 66.1).
Murray Valley Encephalitis Virus
Murray Valley encephalitis virus is carried by the Culex mosquito and is endemic to Northern Australia and Guinea (see Fig. 66.1A). It mostly has occurred in outbreaks with case numbers in the teens to low hundreds, making it much less of a threat than most other flaviviruses. Four outbreaks may have occurred in the early part of the 20th century under the moniker “Australian X” disease, and in 1951, the virus was isolated during the first documented Murray Valley encephalitis virus outbreak. Subsequent outbreaks occurred in 1956, 1974, and 2011. There have been sporadic cases additionally. A study conducted immediately after the 2011 outbreak demonstrated 2.2% seroprevalence in endemic areas, with higher numbers coming from those born before 1974.
Incubation time averages 2 weeks. The vast majority of cases are asymptomatic or gives rise to a mild febrile illness with headache that does not come to medical attention. About 1 out of 150 to 1,000 infections develop more severe symptoms several days later of lethargy, encephalopathy, and occasionally seizures that can progress to brain stem symptoms, flaccid paralysis due to myelitis, and death. The case fatality rate is 15% to 30%, and about 30% to 50% suffer long-term neurologic deficits (see Table 66.1).
In severe cases, T2-weighted MRI of the brain shows bilateral thalamic and brain stem hyperintensities. Pathologically, virus has been recovered from brain tissue, and additionally, there is a striking widespread reactive inflammatory infiltrate throughout the gray matter.
Diagnosis is often by serology, suggesting that specific Murray Valley encephalitis virus IgM appears several days after infection and persists for months. Antibodies can also be evaluated in CSF, as well, and there are Murray Valley encephalitis virus RNA assays for detection in serum. Management is supportive.
St. Louis Encephalitis Virus
St. Louis encephalitis virus is carried by Culex species mosquitoes and is a cause of epidemic encephalitis in both North and South America but mostly in the United States (see Fig. 66.1B). Epidemics typically occur during the summer season. The vast majority of individuals have asymptomatic infections. Otherwise, presenting symptoms mimic a flulike illness and include fever, headache, and lethargy. Neurologic features can include seizures, ataxia, confusion, hemiparesis, and myoclonus.
CSF analysis demonstrates a predominantly lymphocytic pleocytosis. St. Louis encephalitis virus is rarely isolated from blood or serum and diagnosis largely requires demonstration of St. Louis encephalitis virus-specific CSF IgM. MRI can show T2-hyperintensities in the basal ganglia and in some cases, abnormal signal is seen within the substantia nigra. Pathology in St. Louis encephalitis virus cases includes perivascular, meningeal, and capillary lymphocytic infiltrates and activated microglia in gray and white matter. There are widespread neuronal degenerative changes, more obvious in cortex, basal ganglia, and cerebellum. A few St. Louis encephalitis virus cases have evidence of inflammation and neuronal loss in the spinal cord.
Treatment is supportive. Mortality varies considerably in case series and has been reported as high as 20%; long-term morbidity occurs in up to 50% of cases (see Table 66.1). Prognosis is worse with those who develop seizures.
Powassan Virus
This flavivirus is carried by the Dermacentor spp. and Ixodes ticks and is endemic in Canada, the northern United States, and parts of Russia (see Fig. 66.1B). It derives its name from the town in Canada where disease was first identified in 1958. Like Murray Valley encephalitis virus and St. Louis encephalitis virus, its epidemiologic significance pales in comparison to other flaviviruses.
Symptoms occur after an incubation period of 1 to 4 weeks and begin with malaise, fever, and pharyngitis but can progress to hemiplegia, vomiting, marked brain stem dysfunction, coma, and death. CSF studies, as with nearly all viral encephalitides, usually demonstrate a moderate lymphocytic pleocytosis and modestly elevated protein concentration. RNA and antibodies can be detected in blood and/or CSF, although the tests are not widely available; referral to state laboratories in the United States is advised.
Pathologic studies demonstrate intense lymphocytic infiltrates and necrosis of gray matter mostly in the basal ganglia, thalamus, and mesial temporal lobes, although involvement is widespread. Neuronal cells demonstrate eosinophilic inclusion bodies. There is no specific therapy for this disease, and treatment is supportive. About half of the survivors suffer permanent sequelae (see Table 66.1).
BUNYAVIRUSES
Bunyaviruses are negative-sense, single-stranded helical RNA viruses that are encapsulated. Although some are arboviruses, several are spread by rodents and are not associated with significant neurologic disease. Those that do result in encephalitis have less epidemiologic significance than most of the flaviviruses, which are found in densely populated areas, are widespread globally, and/or are much more neurovirulent.
Lacrosse Virus
Lacrosse virus is transmitted by the Aedes triseriatus mosquito. Lacrosse virus is endemic to the United States, and symptomatic cases are most commonly seen across the Ohio River Valley, mid-Atlantic, and Midwest. In these areas, the incidence is about 10 to 30 per 100,000 population but only about 0.3% to 4% are symptomatic. Most cases are reported in children, with only about 3% occurring beyond the age of 20 years.
Initial infection causes viral replication in muscle followed by viremia and CNS invasion. The mechanism of entry into the CNS is unknown, but neurons and glial cells in the frontal, temporal, and parietal lobes are mostly affected. Presentation is of headache and fever, which progresses over days to seizures and encephalopathy about 25% to 50% of the time. CSF demonstrates a lymphocytic pleocytosis with modestly elevated protein concentration, although results can be entirely normal. Lacrosse virus IgM in CSF is diagnostic; otherwise, diagnosis comes from fourfold increase in IgG antibody titers from acute to convalescent phase. Alternatively, antigen detection on biopsy specimen provides the diagnosis. Treatment is supportive and the disease monophasic; mortality is less than 1%.
Jamestown Canyon Virus
This virus infects many species of mosquitoes and flies and is found throughout the United States into Canada. It is an extremely rare cause of mild meningoencephalitis, with less than a score of cases reported. However, seroprevalence has been reported as high as 27%, suggesting neurovirulence is very low. Symptoms mirror those of other arboviruses, with onset of a mild febrile illness followed by severe headaches. Serologic studies are diagnostic when a fourfold rise in IgG is seen between acute and convalescent phases; treatment is supportive.
REOVIRUSES
Reoviruses are a family of double-stranded, nonenveloped RNA viruses with icosahedral capsids. As with bunyaviruses, these infections are considerably more isolated than most flavivirus infections.
This Reoviridae genus includes Colorado tick fever virus, California hare coltivirus, Salmon River virus, and the European Eyach virus. All are associated with human disease, but Colorado tick fever virus causes the majority of human infections. It is carried by Dermacentor andersoni ticks and is mostly seen in the Rocky Mountains and western United States into Canada at elevations of 4,000 to 10,000 feet. Men are more often infected than women, likely due to lifestyle characteristics leading to exposure. There have been some 200 to 300 cases reported, but the incidence is likely much higher, as most infections are thought to be asymptomatic. Presentation after an incubation period of about 3 to 5 days is of acute fever, headache, nausea, myalgias, and in some, a maculopapular rash. About a week later, a meningoencephalitis may develop (mostly children). There can be additional systemic involvement of the heart, liver, testes, epididymis, and lungs. Only a couple of deaths have been reported, and these have been due to hemorrhagic shock complicating disease. This monophasic illness resolves after another week.
CSF often shows a lymphocytic pleocytosis and modestly elevated protein concentration. Diagnosis is made by viral isolation from blood or CSF or serologies and treatment is supportive, with special care to avoid antiplatelet agents given the potential for hemorrhagic complications.
TOGAVIRUSES
Togaviruses are positive-sense, single-stranded, enveloped viruses with icosahedral capsids. There are two genera: Alphavirus and Rubivirus. Alphavirus species are arboviruses, whereas Rubivirus contains rubella, which is transmitted via droplet or mother-child transmission.
Alphavirus (Equine Encephalitis)
There are three types of equine encephalitis, all belonging to the genus Alphavirus, that occur in the Americas (see Fig. 66.1A): Eastern equine encephalitis (EEE), Western equine encephalitis (WEE), and Venezuelan equine encephalitis (VEE). These viruses affect horses primarily but in 1938 were found to cause human disease in those having close contact with affected animals.
Only gold members can continue reading. Log In or Register to continue