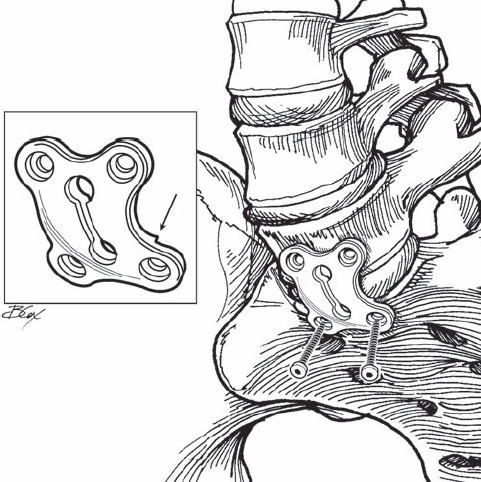
49 Thomas N. Scioscia and Jeffrey C. Wang Recent advances in plating systems have made anterior fixation possible after anterior lumbar interbody placement. Following a supine retroperitoneal or transperitoneal approach, diskectomy is performed and end plates are prepared to bleeding bone. The anterior lumbar interbody fusion (ALIF) graft of choice is then press-fit into the interspace, and fixation is achieved with a low-profile conventional or locking plate. After meticulous hemostasis, abdominal closure is performed. Anterolateral plating is performed through a lateral retroperitoneal approach. After exposure and corpectomy, a structural graft or cage is placed to re-create lordosis. A low-profile conventional or locking contoured plate is then applied laterally with two screws in the superior and inferior vertebral bodies. Fusion rates of stand-alone ALIF have been extensively studied, and pseudarthrosis rates have been reported up to 35%. This may be due to the loss of the anterior longitudinal ligament, which increases instability in the flexion/extension plane. The advent of BMP has also raised the concern of remodeling and weakening of femoral ring allografts. These problems have prompted surgeons to back up ALIF procedures with either standard or percutaneous pedicle screws. Anterior plates have been studied in vitro, and they restore the anterior tension band and sagittal stability. The risk of vascular injury tempered the early excitement about anterior lumbar plating, but newer designs have rekindled interest. The Pyramid plate (Medtronic, Memphis, TN) is specially shaped to fit below the bifurcation of the great vessels and has a cover plate to prevent screw back-out (Fig. 49.1). The anterior tension band (ATB) plate (Synthes Inc, West Chester, PA) is a very low profile plate (3.5 mm), and the screws lock into the plate, minimizing the risk of vascular erosion (Fig. 49.2). Fig. 49.1 Pyramid plate (Medtronic) placed at the L5-S1 interspace. Fig. 49.2 The anterior tension band (ATB) plate (Synthes Inc.) placed at the L5-S1 interspace. Supplemental fixation after ALIF for discogenic back pain with positive diskogram, instability or grade one spondylolisthesis, and pseudarthrosis after failed posterior surgery. The Pyramid plate is indicated only at the L5-S1 disk level. The plate is indicated from L1 to S1, though it should be placed anterolaterally above L5-S1 and used with extreme caution at these higher levels. Supplemental fixation after ALIF for revision of failed spine arthroplasty. Instability with greater than 25% listhesis in any direction. Low-lying bifurcation of the great vessels. Great vessel anatomy must be visualized on magnetic resonance imaging (MRI). The bifurcation should be located superior to the L5 vertebral body when plating the L5-S1 interspace. If this is not the case, consent for posterior instrumentation should be obtained. Calcified great vessels visualized on preoperative radiographs should be retracted carefully to minimize the risk of a thrombotic event with catastrophic consequence. Pulse oximetry placed on the left second toe can alert the surgeon to the need for emergent thrombectomy of the left lower extremity vessels. A retroperitoneal approach is favored over a transperi-toneal approach. The transperitoneal approach is associated with a five- to 10-fold increase in retrograde ejaculation as a complication. Placement of the conventional Pyramid plate needs to be flush on both vertebral bodies because it relies on friction with the screw/plate/bone interface for fixation. This implies that all osteophytes must be removed and the plate may not be ideal with spondylolisthesis. The locking plate is a fixed angle device and it still affords stability even if the plate is not fully seated on bone. When placing the ATB plate at all levels above L5-S1, careful attention must be paid to the great vessels. An experienced vascular surgeon minimizes the risk of vascular injury during the approach. The placement of the interbody graft should be recessed a few millimeters in the disk space. Lateral fluoroscopy is helpful in identifying the disk space margins as the implant is seated and is useful to guide plate and screw placement. The osteophytes should be rongeured before plate placement to ensure maximum bony contact. The smallest plate possible should be used to minimize the risk of vascular erosion. Placement of the plate should be away from the vessels, avoiding direct placement under venous structures. A Pfannenstiel incision or a small left-side oblique incision is made, and the retroperitoneal approach is utilized to access the L5-S1 disk space. The middle sacral artery located in the midline is ligated. The diskectomy includes all of the nucleus, end plates, the anterior annulus, and the ALL. Trial spacers are then impacted to a press-fit position. The implant is then packed with bone graft or bone morphogenetic protein (BMP) and is impacted into the disk space a few millimeters deep to the anterior vertebral body. The plates are sized using the smallest plate that will gain screw purchase into L5 and the sacral promontory. The L5-S1 plate has a cutout for the promontory, which is located on the inferior aspect of the plate. The correct-size plate is then placed on the interspace with all four threaded screw guides attached to the plate. Temporary fixation pins are placed in the contralateral screw holes, and fluoroscopy is used to confirm the correct plate position (Fig. 49.3). The awl is used to prepare the remaining two screw holes through the threaded drill guide. The thread drill guides are removed, the depth gauge is then pushed through the cancellous bone, and the unicortical depth is measured. The screws are then placed and locked into the plate. The temporary pins are removed and the remaining screws are placed in a similar manner. For levels above L5-S1, the plate may need to be placed anterolaterally for better fit around the vessels. An alternative approach for compression may be performed by placing the two inferior screws first. A Schanz pin is placed in L5, and compression forceps are applied to the plate and the pin (Fig. 49.4). The superior screws are then inserted in the previously described manner.
Anterior and Anterolateral Lumbar Fixation Plating
Description
Expectations

Indications
Relative Indications
Contraindications
Relative Contraindications
Special Considerations
Tips, Pearls, and Lessons Learned
Key Procedural Steps
Direct Anterior Approach with the ATB Plate

Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


