14
Anterior Cervical Diskectomy and Foraminotomy
Kern Singh, Alexander R. Vaccaro, Todd J. Albert, and Peter M. Fleischut
Description
Pathologic processes, including trauma and age-related degeneration, may affect the cervical spine, resulting in the clinical presentation of radiculopathy or myelopathy. Anterior cervical diskectomy and foraminotomy is an effective technique for neural decompression secondary to herniated disks and spondylotic spurs.
Key Principles
Adequate neural decompression via a diskectomy requires a precise annulotomy, thorough diskectomy, and meticulous foraminotomy.
Expectations
A thorough diskectomy and meticulous end-plate preparation facilitate neural decompression, disk space distraction, and successful interbody graft incorporation.
Indications
Failure of nonoperative treatment to relieve persistent or recurrent radicular arm pain, progressive neurologic deficit, and myelopathy.
Contraindications
Bleeding disorders and posterior neural compression secondary to hyperlordosis, ligamentous infolding, and osteophytic formation.
Special Considerations
Preoperative imaging is essential to determine the etiologic and anatomic sites of neural compression. Plain radiographs, in addition to magnetic resonance imaging (MRI), myelography, or postmyelogram computed tomography (CT) imaging, are essential for identifying sites of neural compression.
Special Instructions, Positioning, and Anesthesia
The operating room table should be placed into a slightly reverse Trendelenburg position allowing for venous drainage. The patient’s neck may be extended by placing a small roll vertically between the scapulae. Caudal traction to the shoulders is gently applied using adhesive tape. Good lighting and the use of loupes or a microscope facilitates the diskectomy and decompression. Total intravenous narcotic anesthesia is utilized, allowing for the measurement of somatosensory evoked potentials, motor evoked potentials, and dermatomal evoked potentials in a specific nerve root distribution.
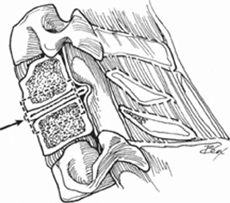
Tips, Pearls, and Lessons Learned
Anatomic landmarks may aid in the placement of the surgical incision. Typically, the hyoid bone overlies the C3 vertebral body, the thyroid cartilage overlies the C4–5 intervertebral disk space, and the cricoid ring overlies the C6 level. Disk space localization is performed with a radiopaque marker and a lateral radiograph (Fig. 14.1). An annulotomy is then made outlining the disk-end-plate junction using a sharp scalpel. Curettes must always stay in the disk space while “peeling” the disk and end-plate cartilage to avoid damaging the esophagus or other soft tissue structures (Fig. 14.2 ). Perforation of the end plate should be avoided to minimize bleeding. A 3-0 angled curette is helpful for getting behind the uncinate process and for creating a path for the 1- and 2-mm Kerrison punch to resect the uncinate process. Adequacy of the foraminotomy can be determined by passing a nerve hook anterior to the exiting nerve root without significant resistance. Routine removal of the posterior longitudinal ligament (PLL) is unnecessary, and there have been reports that postoperative epidural hematoma and other complications may occur with this technique.
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


