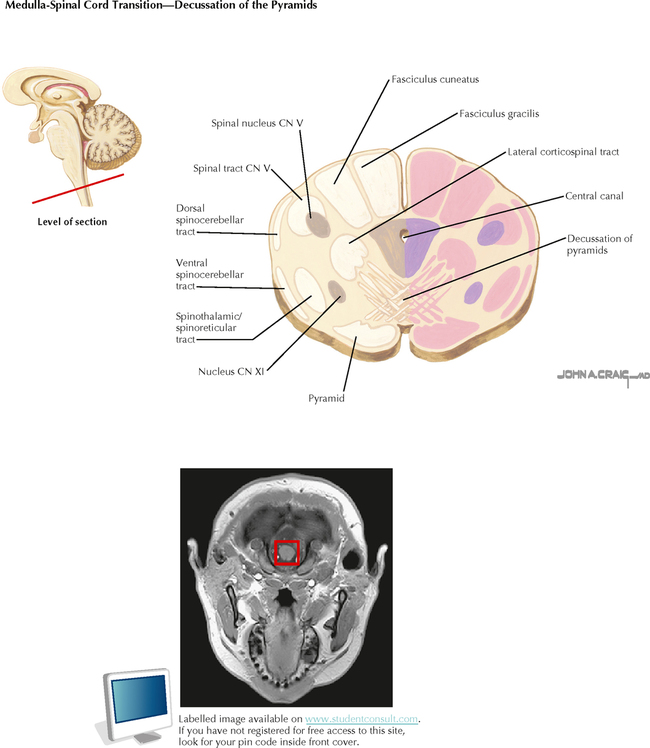
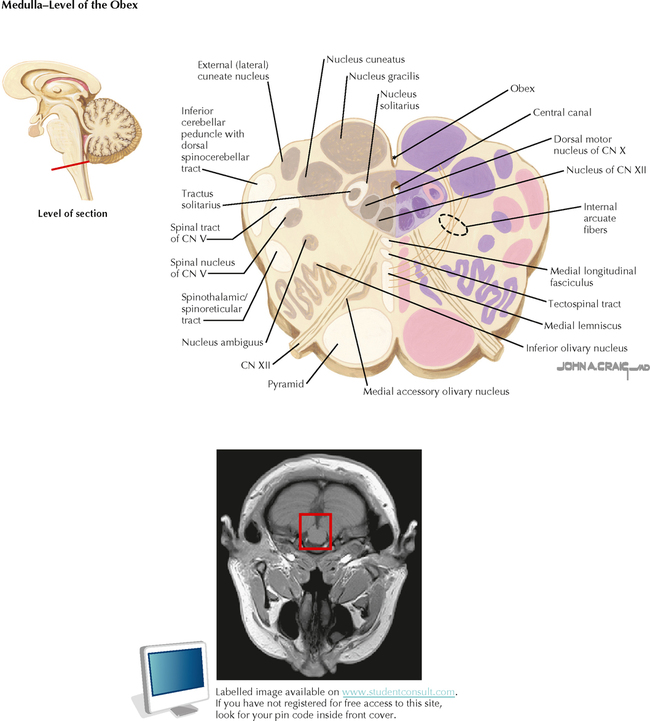
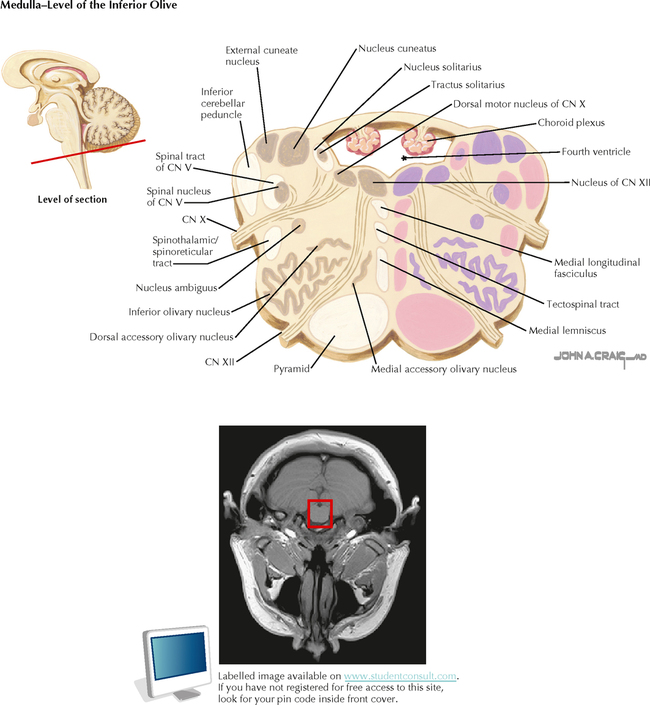
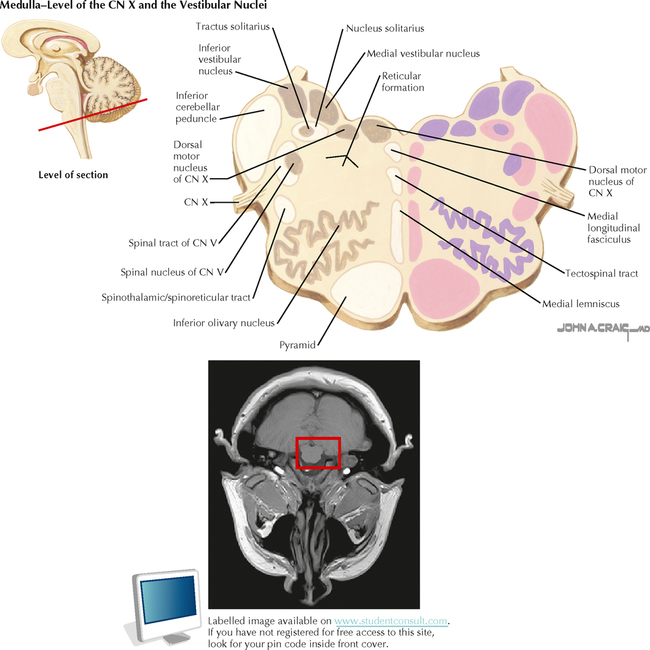
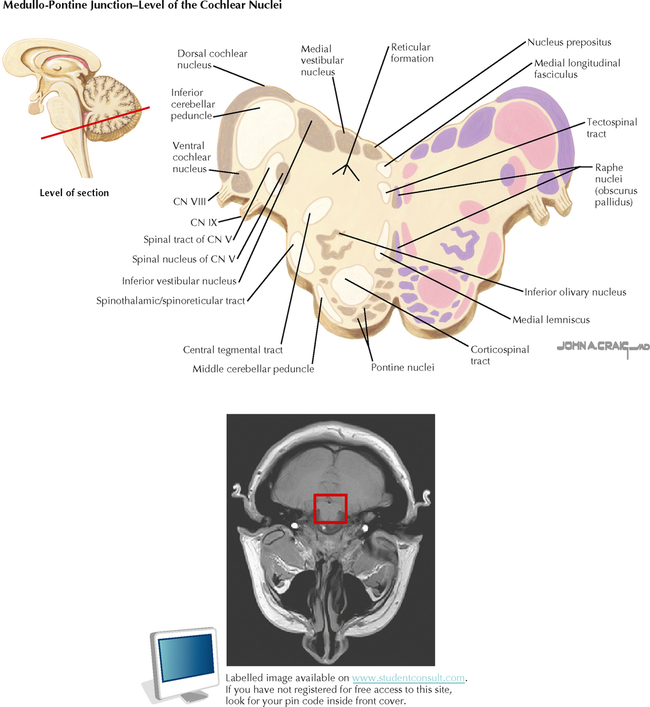
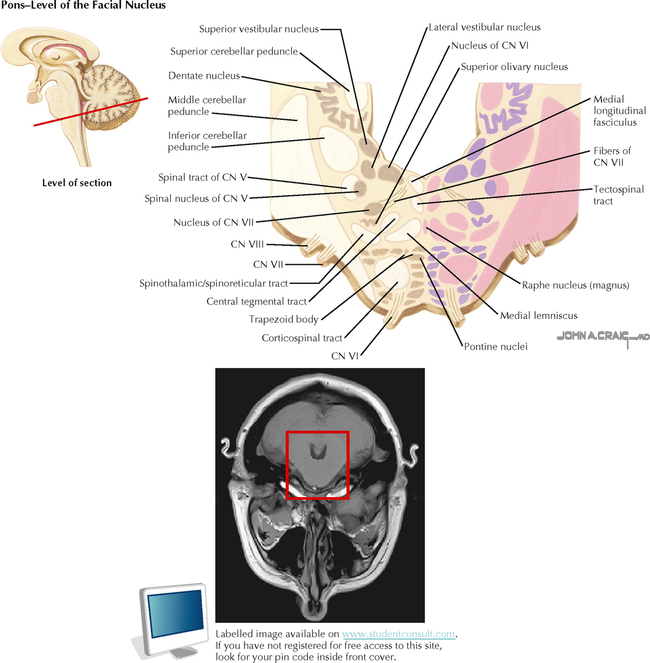
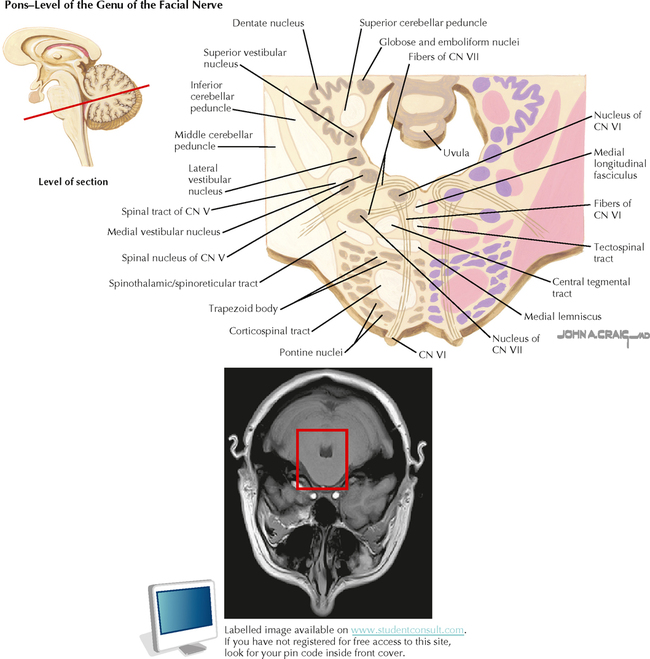
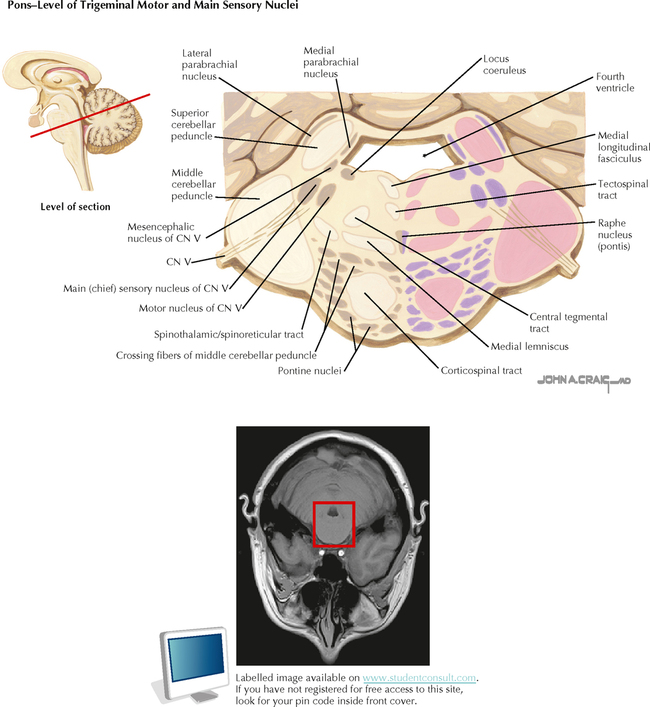
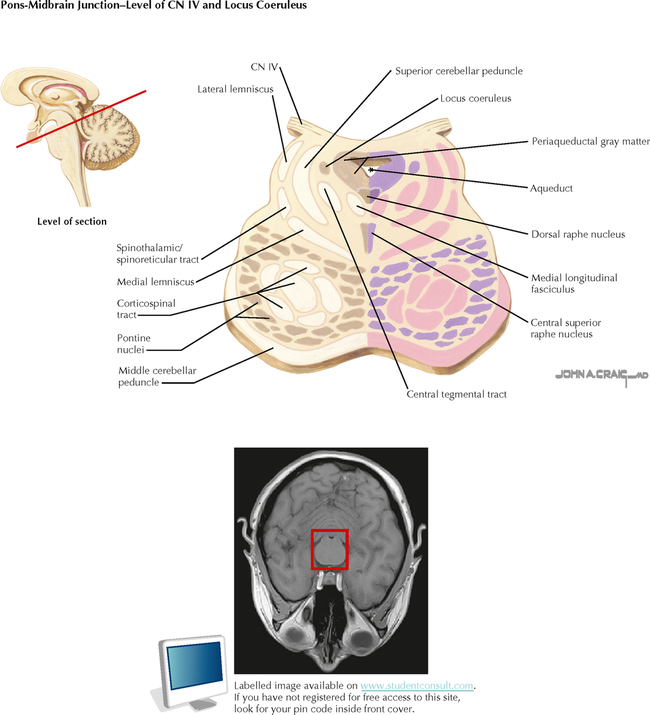
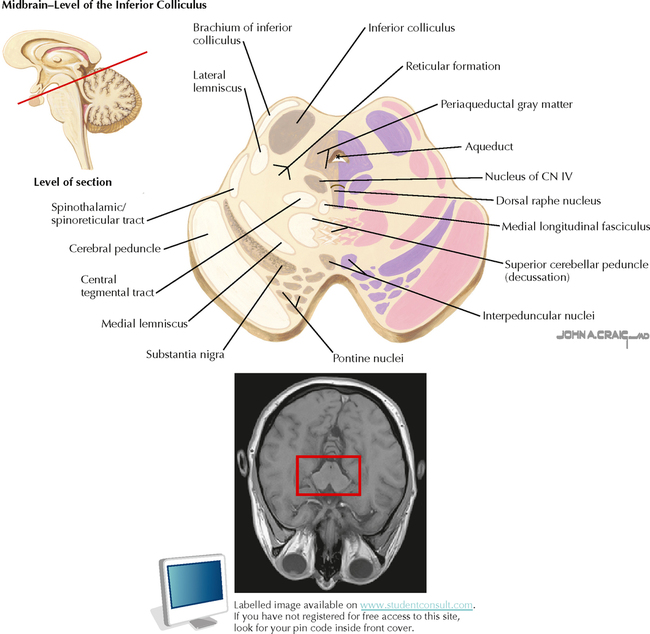
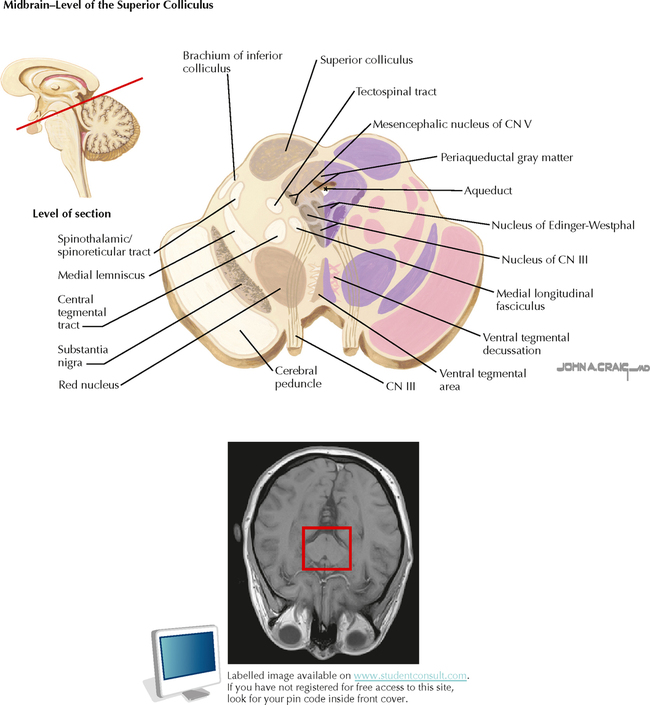
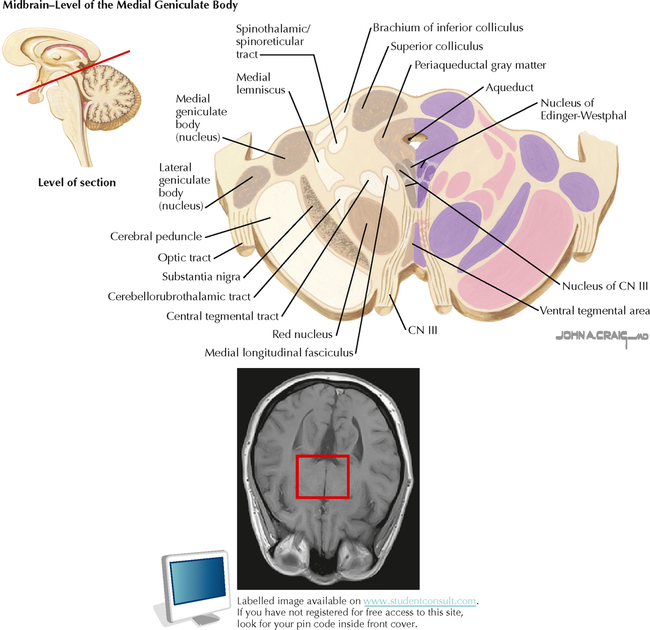
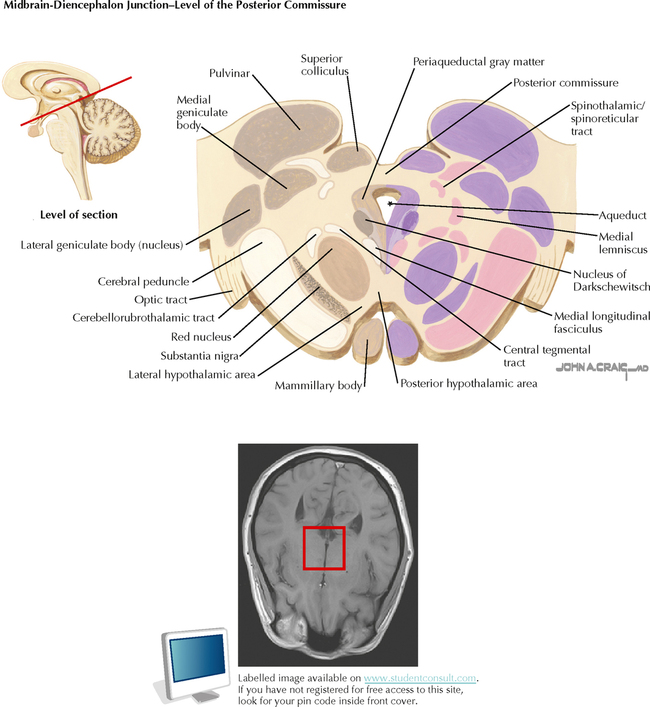
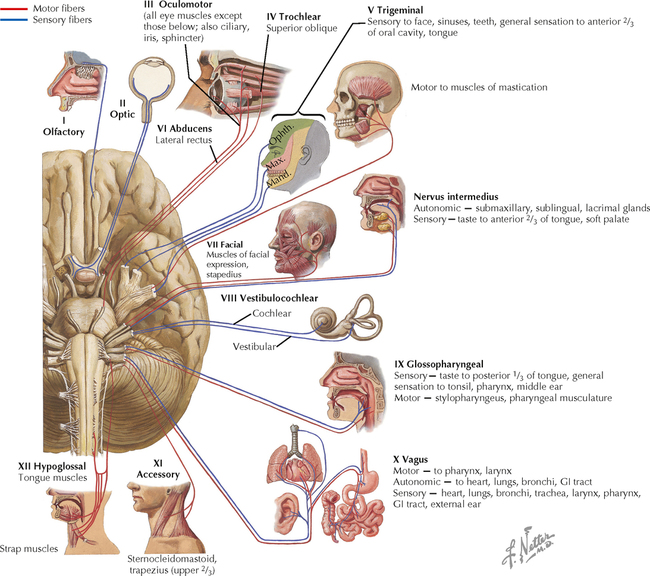
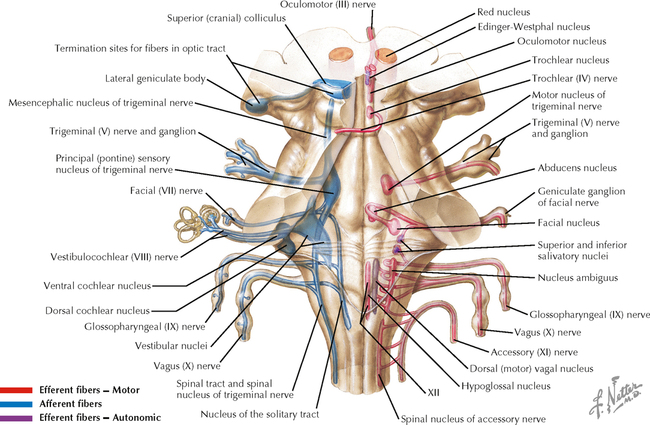
11 BRAIN STEM AND CEREBELLUM Brain Stem Cross-Sectional Anatomy 11.1. Brain Stem Cross-Sectional Anatomy: Section 1 11.2. Brain Stem Cross-Sectional Anatomy: Section 2 11.3. Brain Stem Cross-Sectional Anatomy: Section 3 11.4. Brain Stem Cross-Sectional Anatomy: Section 4 11.5. Brain Stem Cross-Sectional Anatomy: Section 5 11.6. Brain Stem Cross-Sectional Anatomy: Section 6 11.7. Brain Stem Cross-Sectional Anatomy: Section 7 11.8. Brain Stem Cross-Sectional Anatomy: Section 8 11.9. Brain Stem Cross-Sectional Anatomy: Section 9 11.10. Brain Stem Cross-Sectional Anatomy: Section 10 11.11. Brain Stem Cross-Sectional Anatomy: Section 11 11.12. Brain Stem Cross-Sectional Anatomy: Section 12 11.13. Brain Stem Cross-Sectional Anatomy: Section 13 11.14. Brain Stem Cross-Sectional Anatomy: Section 14 Cranial Nerves and Cranial Nerve Nuclei 11.15. Cranial Nerves: Schematic of Distribution of Sensory, Motor, and Autonomic Fibers 11.16. Cranial Nerves and Their Nuclei: Schematic View from Above 11.17. Cranial Nerves and Their Nuclei: Schematic Lateral View 11.18. Nerves of the Orbit 11.19. Nerves of the Orbit 11.20. Extraocular Nerves (III, IV, and VI) and the Ciliary Ganglion: View in Relation to the Eye 11.21. Trigeminal Nerve (V) 11.22. Innervation of the Teeth 11.23. Facial Nerve (VII) 11.24. Facial Nerve Branches and the Parotid Gland 11.25. Vestibulocochlear Nerve (VIII) 11.26. Glossopharyngeal Nerve (IX) 11.27. Accessory Nerve (XI) 11.28. Vagus Nerve (X) 11.29. Hypoglossal Nerve (XII) Reticular Formation 11.30. Reticular Formation: General Pattern of Nuclei in the Brain Stem. 11.31. Reticular Formation: Nuclei and Areas in the Brain Stem and Diencephalon 11.32. Major Afferent and Efferent Connections to the Reticular Formation 11.33. Sleep-Wakefulness Control Cerebellum 11.34. Cerebellar Organization: Lobes and Regions 11.35. Cerebellar Anatomy: Lobules 11.36. Cerebellar Anatomy: Deep Nuclei and Cerebellar Peduncles BRAIN STEM CROSS-SECTIONAL ANATOMY 11.1 BRAIN STEM CROSS-SECTIONAL ANATOMY: SECTION 1 Illustrations of brain stem cross-sections (11.1 through 11.14) are arranged from caudal to rostral, from the spinal-medullary junction to the rostral mesencephalon-diencephalon junction; T1-weighted magnetic resonance images of the brain stem and surrounding tissue are provided for each level. CN, cranial nerve. 11.2 BRAIN STEM CROSS-SECTIONAL ANATOMY: SECTION 2 CLINICAL POINT Several groups of LMNs are present in the lower brain stem, including those supplying the tongue (CN XII), the pharynx and larynx (nucleus ambiguus), and the face (CN VII). Neurodegeneration of these brain stem LMNs can occur in bulbar polio, amyotrophic lateral sclerosis, and other LMN diseases. The affected muscles are atrophic and flaccid. Such a condition is called bulbar palsy (or progressive bulbar paralysis), an LMN disorder, accompanied by loss of movement, tone, and reflexes. The tongue is weak and atrophic, and the patient cannot speak or vocalize (dysarthria or anarthria, not aphasia) and cannot swallow (dysphagia); as a consequence the patient may aspirate in an attempt to swallow. This LMN condition must be distinguished from UMN lesions which, when bilateral, can also result in dysphonia, dysphagia, and weakened bulbar muscles. This UMN condition is called pseudobulbar palsy or spastic bulbar palsy. In this condition, the muscles are not atrophic, and reflexes (jaw jerk and facial reflexes) are brisk. In amyotrophic lateral sclerosis, both LMN and UMN degeneration may occur progressively during the course of the disease. Because the LMNs are the final common pathway to the muscles, the LMN state usually progresses; once the LMNs have degenerated, continuing UMN damage does not make a difference functionally. 11.3 BRAIN STEM CROSS-SECTIONAL ANATOMY: SECTION 3 11.4 BRAIN STEM CROSS-SECTIONAL ANATOMY: SECTION 4 CLINICAL POINT The medulla is supplied with blood by the paramedian and circumferential branches of the anterior spinal artery and the vertebral arteries. A major circumferential branch of the vertebral artery, the posterior inferior cerebellar artery supplies a lateral wedge of medulla with blood. A brain stem stroke or an infarct in a vertebral artery or in the posterior inferior cerebellar artery produces a complex of symptoms called the lateral medullary syndrome (Wallenberg syndrome), which is caused by damage to an array of nuclei and tracts. The patient can demonstrate (1) loss of pain and temperature sensation on the ipsilateral side of the face (descending nucleus and tract of V) and the contralateral side of the body (spinothalamic/spinoreticular system); (2) dysphagia and dysarthria (paralysis of ipsilateral pharyngeal and laryngeal muscles resulting from damage to the ipsilateral nucleus ambiguus); (3) ataxia of the limbs and falling to the ipsilateral side (inferior cerebellar peduncle and its afferent tracts); (4) vertigo with nausea, vomiting, and nystagmus (vestibular nuclei); and (5) ipsilateral Horner’s syndrome, with ptosis, miosis, and anhidrosis (descending axons from the hypothalamus to the T1–T2 intermediolateral cell column of the spinal cord). 11.5 BRAIN STEM CROSS-SECTIONAL ANATOMY: SECTION 5 11.6 BRAIN STEM CROSS-SECTIONAL ANATOMY: SECTION 6 CLINICAL POINT Occlusion of a paramedian branch of the basilar artery in the lower pons results in medial inferior pontine syndrome. This vascular syndrome causes (1) contralateral hemiparesis (corticospinal system) and contralateral drooping of the lower face (corticobulbar fibers); (2) loss of fine, discriminative touch, vibratory sensation, and joint position sense on the contralateral body that is more severe in the upper extremity (medial lemniscus); (3) limb ataxia and gait ataxia (pontine nuclei and bilateral crossing connections going into the middle cerebellar peduncles); (4) paralysis of lateral gaze by the ipsilateral eye, with diplopia (abducens nerve, nucleus); (5) paralysis of conjugate gaze to ipsilateral side, with preservation of convergence (parapontine reticular formation); and (6) diplopia on attempted lateral gaze to the contralateral side, called internuclear ophthalmoplegia (medial longitudinal fasciculus). 11.7 BRAIN STEM CROSS-SECTIONAL ANATOMY: SECTION 7 11.8 BRAIN STEM CROSS-SECTIONAL ANATOMY: SECTION 8 CLINICAL POINT The pons is a common site for a hemorrhagic stroke. A pontine hemorrhage is commonly large and lethal. When not fatal, such a hemorrhage may result in the rapid progression of (1) total paralysis (quadriplegia); (2) decerebrate posturing (extensor posturing) caused by UMN damage to the corticospinal and rubrospinal systems, thereby disinhibiting the lateral vestibular nuclei; (3) coma; (4) paralysis of ocular movements; and (5) small but reactive pupils. A pontine hemorrhage that results in coma is commonly lethal. A large infarct in the basilar artery may produce the same clinical picture. Some small, lacunar infarcts also may occur in the pons; these infarcts may produce purely motor symptoms (contralateral UMN paresis at base of pons), ataxia, or both (cerebellar peduncles, pontine nuclei). 11.9 BRAIN STEM CROSS-SECTIONAL ANATOMY: SECTION 9 CLINICAL POINT A vascular lesion of circumferential branches of the basilar artery or the anterior inferior cerebellar artery can cause lateral pontine syndrome, which is characterized by (1) contralateral loss of sensation in the body, both epicritic and protopathic (medial lemniscus and anterolateral system); (2) loss of pain and temperature sensation on the contralateral face (ventral trigeminal lemniscus, located on dorsal surface of the medial lemniscus); (3) loss of fine, discriminative touch (main sensory nucleus of CN V) or impaired general sensation (CN V fibers) on the ipsilateral face; (4) ipsilateral paralysis of muscles of mastication (motor nucleus of CN V); (5) limb ataxia (middle and superior cerebellar peduncles); (6) paralysis of conjugate gaze to the ipsilateral side (parapontine reticular formation and its connections); and (7) other possible ipsilateral brain stem problems, depending on the extent of the vascular involvement, such as deafness or tinnitus (auditory nuclei or nerve fibers); vertigo and nystagmus (vestibular nuclei or nerve fibers); facial palsy (CN VII nucleus or nerve fibers); and Horner’s syndrome (descending hypothalamo-spinal sympathetic connections). 11.10 BRAIN STEM CROSS-SECTIONAL ANATOMY: SECTION 10 11.11 BRAIN STEM CROSS-SECTIONAL ANATOMY: SECTION 11 CLINICAL POINT A space-occupying lesion in the forebrain, such as a bleed (epidural or subdural hematoma), a tumor, or increased intracranial pressure resulting from a variety of causes, can cause herniation of the forebrain through the tentorium cerebelli. This transtentorial herniation displaces the thalamus and upper midbrain in a downward direction and causes a variety of changes in brain function. These changes are characterized by functions attributable to the remaining intact lower midbrain and more caudal structures, with loss of function of the upper midbrain and more rostral structures. Most conspicuous is a progressive deterioration of the state of consciousness, rapidly going from drowsiness to stupor to an unarousable state of coma; consciousness requires an intact brain stem reticular formation and at least one functioning cerebral hemisphere. When both hemispheres are nonfunctional, coma ensues. With the loss of activity in the corticospinal system and the rubrospinal system and removal of cortical influence on the other UMN pathways, a state of decerebration occurs (called decerebrate rigidity, although it is really spasticity, not true rigidity). The neck is extended (opisthotonus), the arms and legs are extended and rotated inward, and the hands, fingers, feet, and toes are flexed. Plantar responses are extensor. Cheyne-Stokes respiration is seen (crescendo-decrescendo breathing), followed at a slightly later stage of damage by shallow hyperventilation. The pupils are midsized and usually unresponsive because of compression of the third nerves against the free edge of the tentorium. Caloric testing or the doll’s-eye maneuver shows no vertical eye movements (visual tectal damage), and the eyes do not move in a conjugate fashion. 11.12 BRAIN STEM CROSS-SECTIONAL ANATOMY: SECTION 12 11.13 BRAIN STEM CROSS-SECTIONAL ANATOMY: SECTION 13 CLINICAL POINT Paramedian regions of the upper midbrain receive their blood supply mainly from branches of the posterior cerebral and posterior communicating arteries. A vascular lesion at this level (Weber’s syndrome) results in damage to the exiting third nerve fibers, the medial and central portions of the cerebral peduncle, and some passing tracts. A supratentorial mass lesion also can cause lateral and downward compression of one cerebral peduncle and the third nerve against the free edge of the tentorium cerebelli, presenting a similar clinical picture. Compression of the cerebral peduncle with possible involvement of the red nucleus on the affected side produces contralateral hemiplegia, rapidly evolving to a spastic state with a plantar extensor response. A central (lower) facial palsy occurs because of damage to corticobulbar fibers, which travel in the cerebral peduncle. An ipsilateral oculomotor palsy also occurs, with the ipsilateral eye deviated laterally and the ipsilateral pupil fixed (unresponsive to light) and dilated because of unopposed actions of the sympathetics. If the lesion involves the substantia nigra, red nucleus, pallidothalamic fibers, or dentatorubral and dentatothalamic fibers, contralateral movement problems may occur, including akinesia, intention tremor, or choreoathetoid movements. Damage to these later structures, with their accompanying contralateral problems, may occur in isolation along with third-nerve damage caused by more distal vascular involvement of the paramedian branches to the upper midbrain (Benedict’s syndrome). 11.14 BRAIN STEM CROSS-SECTIONAL ANATOMY: SECTION 14 CRANIAL NERVES AND CRANIAL NERVE NUCLEI 11.15 CRANIAL NERVES: SCHEMATIC OF DISTRIBUTION OF SENSORY, MOTOR, AND AUTONOMIC FIBERS CNs I and II, both sensory, are tracts of the central nervous system (CNS) that are derived from the neural tube and myelinated by oligodendroglia. CNs III–XII emerge from the brain stem and supply sensory (CNs V, VII–X); motor (CNs III–VII and IX–XII); and autonomic (CNs III, VII, IX, X) nerve fibers to structures in the head and neck. All of the CNs that emerge from the brain stem distribute ipsilaterally to their target structures. With the exception of CN nucleus IV (trochlear) and some motor components of CN nucleus III (oculomotor), the CN nuclei are located ipsilateral to the point of emergence of the CN. The spinal accessory portion of CN XI emerges from motor neurons in the rostral spinal cord; it ascends through the foramen magnum and then exits with CNs IX and X; thus it is considered a CN. CLINICAL POINT Multiple CNs can be affected by some pathological conditions, such as tumors and granulomas, brain stem infarcts, leptomeningeal carcinomatosis, and aneurysms. Extramedullary pathology affects mainly the sensory, motor, and autonomic components of the involved CNs: internal pathology in the brain stem also involves the long tracts. An aneurysm in the cavernous sinus may involve CNs III–VI. A large tumor in the middle cranial fossa in the retrosphenoid space may affect cranial nerves III–VI. A large tumor in the cerebellopontine angle involves CNs VII and VIII and sometimes expands to involve V and IX. Tumors and aneurysms in the jugular foramen may involve CNs IX, X, and XI. Granulomatous lesions such as sarcoids in the posterior retroparotid space may affect cranial nerves IX–XII as well as the sympathetic nerves to the head. 11.16 CRANIAL NERVES AND THEIR NUCLEI: SCHEMATIC VIEW FROM ABOVE Only gold members can continue reading. Log In or Register to continue Share this:Click to share on Twitter (Opens in new window)Click to share on Facebook (Opens in new window) Related Related posts: VENTRICLES AND THE CEREBROSPINAL FLUID SPINAL CORD MOTOR SYSTEMS AUTONOMIC-HYPOTHALAMIC-LIMBIC SYSTEMS TELENCEPHALON PERIPHERAL NERVOUS SYSTEM Stay updated, free articles. Join our Telegram channel Join Tags: Netters Atlas of Neuroscience with STUDENT CONSULT Online Access Jun 4, 2016 | Posted by admin in NEUROLOGY | Comments Off on BRAIN STEM AND CEREBELLUM Full access? Get Clinical Tree
11 BRAIN STEM AND CEREBELLUM Brain Stem Cross-Sectional Anatomy 11.1. Brain Stem Cross-Sectional Anatomy: Section 1 11.2. Brain Stem Cross-Sectional Anatomy: Section 2 11.3. Brain Stem Cross-Sectional Anatomy: Section 3 11.4. Brain Stem Cross-Sectional Anatomy: Section 4 11.5. Brain Stem Cross-Sectional Anatomy: Section 5 11.6. Brain Stem Cross-Sectional Anatomy: Section 6 11.7. Brain Stem Cross-Sectional Anatomy: Section 7 11.8. Brain Stem Cross-Sectional Anatomy: Section 8 11.9. Brain Stem Cross-Sectional Anatomy: Section 9 11.10. Brain Stem Cross-Sectional Anatomy: Section 10 11.11. Brain Stem Cross-Sectional Anatomy: Section 11 11.12. Brain Stem Cross-Sectional Anatomy: Section 12 11.13. Brain Stem Cross-Sectional Anatomy: Section 13 11.14. Brain Stem Cross-Sectional Anatomy: Section 14 Cranial Nerves and Cranial Nerve Nuclei 11.15. Cranial Nerves: Schematic of Distribution of Sensory, Motor, and Autonomic Fibers 11.16. Cranial Nerves and Their Nuclei: Schematic View from Above 11.17. Cranial Nerves and Their Nuclei: Schematic Lateral View 11.18. Nerves of the Orbit 11.19. Nerves of the Orbit 11.20. Extraocular Nerves (III, IV, and VI) and the Ciliary Ganglion: View in Relation to the Eye 11.21. Trigeminal Nerve (V) 11.22. Innervation of the Teeth 11.23. Facial Nerve (VII) 11.24. Facial Nerve Branches and the Parotid Gland 11.25. Vestibulocochlear Nerve (VIII) 11.26. Glossopharyngeal Nerve (IX) 11.27. Accessory Nerve (XI) 11.28. Vagus Nerve (X) 11.29. Hypoglossal Nerve (XII) Reticular Formation 11.30. Reticular Formation: General Pattern of Nuclei in the Brain Stem. 11.31. Reticular Formation: Nuclei and Areas in the Brain Stem and Diencephalon 11.32. Major Afferent and Efferent Connections to the Reticular Formation 11.33. Sleep-Wakefulness Control Cerebellum 11.34. Cerebellar Organization: Lobes and Regions 11.35. Cerebellar Anatomy: Lobules 11.36. Cerebellar Anatomy: Deep Nuclei and Cerebellar Peduncles BRAIN STEM CROSS-SECTIONAL ANATOMY 11.1 BRAIN STEM CROSS-SECTIONAL ANATOMY: SECTION 1 Illustrations of brain stem cross-sections (11.1 through 11.14) are arranged from caudal to rostral, from the spinal-medullary junction to the rostral mesencephalon-diencephalon junction; T1-weighted magnetic resonance images of the brain stem and surrounding tissue are provided for each level. CN, cranial nerve. 11.2 BRAIN STEM CROSS-SECTIONAL ANATOMY: SECTION 2 CLINICAL POINT Several groups of LMNs are present in the lower brain stem, including those supplying the tongue (CN XII), the pharynx and larynx (nucleus ambiguus), and the face (CN VII). Neurodegeneration of these brain stem LMNs can occur in bulbar polio, amyotrophic lateral sclerosis, and other LMN diseases. The affected muscles are atrophic and flaccid. Such a condition is called bulbar palsy (or progressive bulbar paralysis), an LMN disorder, accompanied by loss of movement, tone, and reflexes. The tongue is weak and atrophic, and the patient cannot speak or vocalize (dysarthria or anarthria, not aphasia) and cannot swallow (dysphagia); as a consequence the patient may aspirate in an attempt to swallow. This LMN condition must be distinguished from UMN lesions which, when bilateral, can also result in dysphonia, dysphagia, and weakened bulbar muscles. This UMN condition is called pseudobulbar palsy or spastic bulbar palsy. In this condition, the muscles are not atrophic, and reflexes (jaw jerk and facial reflexes) are brisk. In amyotrophic lateral sclerosis, both LMN and UMN degeneration may occur progressively during the course of the disease. Because the LMNs are the final common pathway to the muscles, the LMN state usually progresses; once the LMNs have degenerated, continuing UMN damage does not make a difference functionally. 11.3 BRAIN STEM CROSS-SECTIONAL ANATOMY: SECTION 3 11.4 BRAIN STEM CROSS-SECTIONAL ANATOMY: SECTION 4 CLINICAL POINT The medulla is supplied with blood by the paramedian and circumferential branches of the anterior spinal artery and the vertebral arteries. A major circumferential branch of the vertebral artery, the posterior inferior cerebellar artery supplies a lateral wedge of medulla with blood. A brain stem stroke or an infarct in a vertebral artery or in the posterior inferior cerebellar artery produces a complex of symptoms called the lateral medullary syndrome (Wallenberg syndrome), which is caused by damage to an array of nuclei and tracts. The patient can demonstrate (1) loss of pain and temperature sensation on the ipsilateral side of the face (descending nucleus and tract of V) and the contralateral side of the body (spinothalamic/spinoreticular system); (2) dysphagia and dysarthria (paralysis of ipsilateral pharyngeal and laryngeal muscles resulting from damage to the ipsilateral nucleus ambiguus); (3) ataxia of the limbs and falling to the ipsilateral side (inferior cerebellar peduncle and its afferent tracts); (4) vertigo with nausea, vomiting, and nystagmus (vestibular nuclei); and (5) ipsilateral Horner’s syndrome, with ptosis, miosis, and anhidrosis (descending axons from the hypothalamus to the T1–T2 intermediolateral cell column of the spinal cord). 11.5 BRAIN STEM CROSS-SECTIONAL ANATOMY: SECTION 5 11.6 BRAIN STEM CROSS-SECTIONAL ANATOMY: SECTION 6 CLINICAL POINT Occlusion of a paramedian branch of the basilar artery in the lower pons results in medial inferior pontine syndrome. This vascular syndrome causes (1) contralateral hemiparesis (corticospinal system) and contralateral drooping of the lower face (corticobulbar fibers); (2) loss of fine, discriminative touch, vibratory sensation, and joint position sense on the contralateral body that is more severe in the upper extremity (medial lemniscus); (3) limb ataxia and gait ataxia (pontine nuclei and bilateral crossing connections going into the middle cerebellar peduncles); (4) paralysis of lateral gaze by the ipsilateral eye, with diplopia (abducens nerve, nucleus); (5) paralysis of conjugate gaze to ipsilateral side, with preservation of convergence (parapontine reticular formation); and (6) diplopia on attempted lateral gaze to the contralateral side, called internuclear ophthalmoplegia (medial longitudinal fasciculus). 11.7 BRAIN STEM CROSS-SECTIONAL ANATOMY: SECTION 7 11.8 BRAIN STEM CROSS-SECTIONAL ANATOMY: SECTION 8 CLINICAL POINT The pons is a common site for a hemorrhagic stroke. A pontine hemorrhage is commonly large and lethal. When not fatal, such a hemorrhage may result in the rapid progression of (1) total paralysis (quadriplegia); (2) decerebrate posturing (extensor posturing) caused by UMN damage to the corticospinal and rubrospinal systems, thereby disinhibiting the lateral vestibular nuclei; (3) coma; (4) paralysis of ocular movements; and (5) small but reactive pupils. A pontine hemorrhage that results in coma is commonly lethal. A large infarct in the basilar artery may produce the same clinical picture. Some small, lacunar infarcts also may occur in the pons; these infarcts may produce purely motor symptoms (contralateral UMN paresis at base of pons), ataxia, or both (cerebellar peduncles, pontine nuclei). 11.9 BRAIN STEM CROSS-SECTIONAL ANATOMY: SECTION 9 CLINICAL POINT A vascular lesion of circumferential branches of the basilar artery or the anterior inferior cerebellar artery can cause lateral pontine syndrome, which is characterized by (1) contralateral loss of sensation in the body, both epicritic and protopathic (medial lemniscus and anterolateral system); (2) loss of pain and temperature sensation on the contralateral face (ventral trigeminal lemniscus, located on dorsal surface of the medial lemniscus); (3) loss of fine, discriminative touch (main sensory nucleus of CN V) or impaired general sensation (CN V fibers) on the ipsilateral face; (4) ipsilateral paralysis of muscles of mastication (motor nucleus of CN V); (5) limb ataxia (middle and superior cerebellar peduncles); (6) paralysis of conjugate gaze to the ipsilateral side (parapontine reticular formation and its connections); and (7) other possible ipsilateral brain stem problems, depending on the extent of the vascular involvement, such as deafness or tinnitus (auditory nuclei or nerve fibers); vertigo and nystagmus (vestibular nuclei or nerve fibers); facial palsy (CN VII nucleus or nerve fibers); and Horner’s syndrome (descending hypothalamo-spinal sympathetic connections). 11.10 BRAIN STEM CROSS-SECTIONAL ANATOMY: SECTION 10 11.11 BRAIN STEM CROSS-SECTIONAL ANATOMY: SECTION 11 CLINICAL POINT A space-occupying lesion in the forebrain, such as a bleed (epidural or subdural hematoma), a tumor, or increased intracranial pressure resulting from a variety of causes, can cause herniation of the forebrain through the tentorium cerebelli. This transtentorial herniation displaces the thalamus and upper midbrain in a downward direction and causes a variety of changes in brain function. These changes are characterized by functions attributable to the remaining intact lower midbrain and more caudal structures, with loss of function of the upper midbrain and more rostral structures. Most conspicuous is a progressive deterioration of the state of consciousness, rapidly going from drowsiness to stupor to an unarousable state of coma; consciousness requires an intact brain stem reticular formation and at least one functioning cerebral hemisphere. When both hemispheres are nonfunctional, coma ensues. With the loss of activity in the corticospinal system and the rubrospinal system and removal of cortical influence on the other UMN pathways, a state of decerebration occurs (called decerebrate rigidity, although it is really spasticity, not true rigidity). The neck is extended (opisthotonus), the arms and legs are extended and rotated inward, and the hands, fingers, feet, and toes are flexed. Plantar responses are extensor. Cheyne-Stokes respiration is seen (crescendo-decrescendo breathing), followed at a slightly later stage of damage by shallow hyperventilation. The pupils are midsized and usually unresponsive because of compression of the third nerves against the free edge of the tentorium. Caloric testing or the doll’s-eye maneuver shows no vertical eye movements (visual tectal damage), and the eyes do not move in a conjugate fashion. 11.12 BRAIN STEM CROSS-SECTIONAL ANATOMY: SECTION 12 11.13 BRAIN STEM CROSS-SECTIONAL ANATOMY: SECTION 13 CLINICAL POINT Paramedian regions of the upper midbrain receive their blood supply mainly from branches of the posterior cerebral and posterior communicating arteries. A vascular lesion at this level (Weber’s syndrome) results in damage to the exiting third nerve fibers, the medial and central portions of the cerebral peduncle, and some passing tracts. A supratentorial mass lesion also can cause lateral and downward compression of one cerebral peduncle and the third nerve against the free edge of the tentorium cerebelli, presenting a similar clinical picture. Compression of the cerebral peduncle with possible involvement of the red nucleus on the affected side produces contralateral hemiplegia, rapidly evolving to a spastic state with a plantar extensor response. A central (lower) facial palsy occurs because of damage to corticobulbar fibers, which travel in the cerebral peduncle. An ipsilateral oculomotor palsy also occurs, with the ipsilateral eye deviated laterally and the ipsilateral pupil fixed (unresponsive to light) and dilated because of unopposed actions of the sympathetics. If the lesion involves the substantia nigra, red nucleus, pallidothalamic fibers, or dentatorubral and dentatothalamic fibers, contralateral movement problems may occur, including akinesia, intention tremor, or choreoathetoid movements. Damage to these later structures, with their accompanying contralateral problems, may occur in isolation along with third-nerve damage caused by more distal vascular involvement of the paramedian branches to the upper midbrain (Benedict’s syndrome). 11.14 BRAIN STEM CROSS-SECTIONAL ANATOMY: SECTION 14 CRANIAL NERVES AND CRANIAL NERVE NUCLEI 11.15 CRANIAL NERVES: SCHEMATIC OF DISTRIBUTION OF SENSORY, MOTOR, AND AUTONOMIC FIBERS CNs I and II, both sensory, are tracts of the central nervous system (CNS) that are derived from the neural tube and myelinated by oligodendroglia. CNs III–XII emerge from the brain stem and supply sensory (CNs V, VII–X); motor (CNs III–VII and IX–XII); and autonomic (CNs III, VII, IX, X) nerve fibers to structures in the head and neck. All of the CNs that emerge from the brain stem distribute ipsilaterally to their target structures. With the exception of CN nucleus IV (trochlear) and some motor components of CN nucleus III (oculomotor), the CN nuclei are located ipsilateral to the point of emergence of the CN. The spinal accessory portion of CN XI emerges from motor neurons in the rostral spinal cord; it ascends through the foramen magnum and then exits with CNs IX and X; thus it is considered a CN. CLINICAL POINT Multiple CNs can be affected by some pathological conditions, such as tumors and granulomas, brain stem infarcts, leptomeningeal carcinomatosis, and aneurysms. Extramedullary pathology affects mainly the sensory, motor, and autonomic components of the involved CNs: internal pathology in the brain stem also involves the long tracts. An aneurysm in the cavernous sinus may involve CNs III–VI. A large tumor in the middle cranial fossa in the retrosphenoid space may affect cranial nerves III–VI. A large tumor in the cerebellopontine angle involves CNs VII and VIII and sometimes expands to involve V and IX. Tumors and aneurysms in the jugular foramen may involve CNs IX, X, and XI. Granulomatous lesions such as sarcoids in the posterior retroparotid space may affect cranial nerves IX–XII as well as the sympathetic nerves to the head. 11.16 CRANIAL NERVES AND THEIR NUCLEI: SCHEMATIC VIEW FROM ABOVE Only gold members can continue reading. Log In or Register to continue Share this:Click to share on Twitter (Opens in new window)Click to share on Facebook (Opens in new window) Related Related posts: VENTRICLES AND THE CEREBROSPINAL FLUID SPINAL CORD MOTOR SYSTEMS AUTONOMIC-HYPOTHALAMIC-LIMBIC SYSTEMS TELENCEPHALON PERIPHERAL NERVOUS SYSTEM Stay updated, free articles. Join our Telegram channel Join Tags: Netters Atlas of Neuroscience with STUDENT CONSULT Online Access Jun 4, 2016 | Posted by admin in NEUROLOGY | Comments Off on BRAIN STEM AND CEREBELLUM Full access? Get Clinical Tree