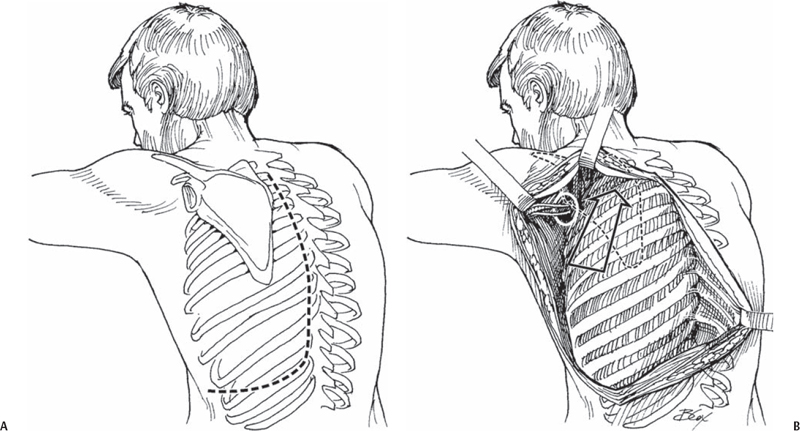
53 Robert M. Campbell, Jr. To lengthen the concave constricted hemithorax through VEPTR expansion thoracoplasty with correction of congenital scoliosis to maximize the potential for thoracic growth to benefit the underlying lungs. With vertical expandable prosthetic titanium rib (VEPTR) expansion thoracoplasty, one can stabilize, or correct, rigid congenital scoliosis, without the growth inhibition effects of spine fusion, and enlarge the constricted concave hemithorax with probable benefit for the underlying lung. The thoracic spine can grow with further increase in thoracic volume. Additional benefits include leveling the shoulders, and improving both head and truncal decompensation. Progressive thoracic congenital scoliosis, in a patient aged 6 months up to skeletal maturity, with three or more fused ribs at the apex of the concave hemithorax, greater than 10% reduction in space available for lung, and having progressive thoracic insufficiency syndrome. Thoracic insufficiency syndrome is identified by the inability of the thorax to support normal respiration or lung growth. Inadequate soft tissue coverage for devices, poor rib bone stock or absence of proximal ribs for attachment of devices, absent diaphragmatic function, active pulmonary infection, or inability to undergo repetitive episodes under general anesthesia. Preoperative magnetic resonance imaging (MRI) of the entire spinal cord is advised to rule out associated spinal cord pathology. An echocardiogram is performed to rule out congenital heart disease, and preopera-tive respiratory syncytial virus screen. Patients are placed in the lateral decubitus position with the operative side upward. Somatosensory evoked potentials and motor evoked potentials of extremities are monitored during surgery. A central line and arterial catheter are recommended. To increase the necessary soft tissue coverage, an oral appetite stimulant, Periactin, tube feeding, or gastric percutaneous endoscopic gastrostomy (PEG) feedings are useful. A body weight at the 25th percentile of normal, or greater, reduces the risk of skin slough over devices. The superior VEPTR cradle site should be placed at the superior aspect of the curve, but not into the flexible spine above it because of the risk of a proximal compensatory curve. Severe lateral contracture of the thorax can be corrected with a Harrington outrigger from a temporary rib cradle attached to chest wall in the posterior axillary line extending down to the lumbar hook site or to the pelvis with a Dunn-McCarthy hook. Acute thoracic outlet syndrome can be encountered with closure because of the altered proximal thoracic anatomy, so both pulse oximeter and upper extremity evoked potentials are monitored for loss of signal, and any changes are addressed by altering closure to let the scapula retract itself more proximal. A modified thoracotomy incision is made with the distal portion carried anteriorly in line with the tenth rib (Fig. 53.1A). The paraspinal muscles are reflected medially to the tips of the transverse processes, with care taken not to damage the rib periosteum (Fig. 53.1B). The VEPTR (Synthes Spine Co., West Chester, PA) is now ready for insertion. The superior VEPTR cradle is first placed adjacent to the tips of the transverse processes of the spine around two ribs or a fused rib mass. Next, the opening wedge thoracostomy is performed at the apex of the fused chest wall. Usually there is a fibrous cleft present anteriorly in the fused ribs in line with the planned thoracostomy. This is released with cautery, with a No. 4 Penfield retractor inserted to protect the underlying pleura, and then the thoracostomy is continued with a Kerrison rongeur, cutting a channel transversely through the rib fusion mass up to the transverse processes (Fig. 53.2A).
Rib Expansion Technique for Congenital Scoliosis
Description
Expectations
Indications
Contraindications
Special Considerations
Special Instructions, Position, and Anesthesia
Tips, Pearls, and Lessons Learned
Key Procedural Steps
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


