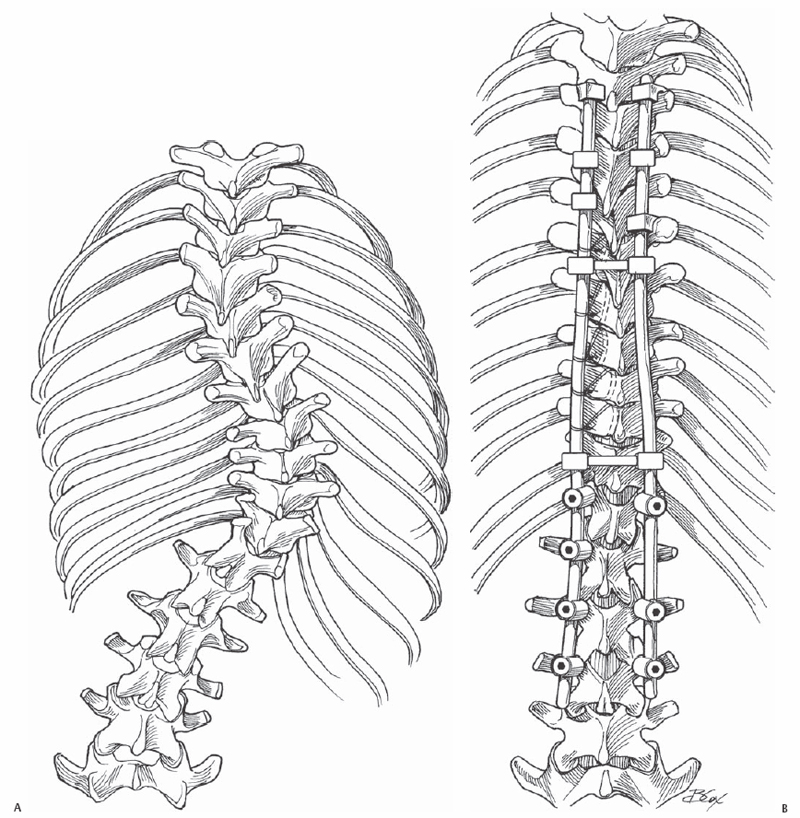
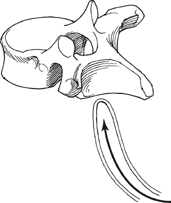
28 Alexios Apazidis, Sanjeev Sabharwal, and Michael J. Vives Sublaminar wires are often used in conjunction with longitudinal members (rods) to provide rigid segment stability to the posterior spine. Sublaminar wires are an efficient means of manipulating the spinal column in the coronal, transverse, and sagittal planes. The risk of bone/implant failure is lessened due to the multitude of points of fixation contact available with this form of instrumentation. Wire placement at the extremes of the instrumentation construct resists implant pullout in the sagittal plane. Sublaminar wire placement is extremely safe in well-trained hands. Substantial translational correction in the coronal plane is possible in flexible scoliotic curves (Fig. 28.1). A recent study demonstrated similar operating times for scoliosis cases using apical sublaminar wires versus pedicle screws. Fig. 28.1(A,B) A patient with scoliosis treated with posterior instrumentation and fusion using apical sublaminar wires. Any multilevel posterior fusion construct with intact posterior elements. Sublaminar wires should not be placed in regions of spinal stenosis, swelling of the neural elements, or levels of posterior element fracture or deficiency. Once the wire is passed, it should be twisted over the respective posterior lamina to prevent inadvertent canal migration. The radius of curvature of the bent sublaminar wire should be at least equal to the width of the lamina. The primary bend can be made over the handle of a Cobb elevator, with a compensatory bend to facilitate wire passage. The wires should be passed just beneath the lamina in a caudal to cranial direction. Central passage of the wires under the lamina avoids the potential for nerve root injury from lateral wire deviation and minimizes the risk of encountering epidural bleeders. The spinous processes of the instrumented vertebrae are removed with a double-action bone cutter to adequately visualize the ligamentum flavum. A thin Leksell rongeur is used to create a midline defect in the ligamentum flavum, which is further enlarged with Kerrison rongeurs to allow safe passage of the sublaminar wire. Develop a routine for wire passage where the inferior tail of the sublaminar wire is placed either medial or lateral to the superior tail at the time of wire bending, prior to twist locking the wire ends. Some favor placing the inferior tail laterally, because the free ends of the wire can puncture the surgeon’s gloves. Remember always to separate the wire ends at the time of rod placement prior to wire tightening to avoid the technical difficulty of trying to slip a wire end between the rod and bone after the wire is well seated. When twist locking the wire ends, rotate the wire ends away from the midline. If wires are placed at levels above or below the instrumentation, they should be twist tightened in a direction away from the fusion mass. For long constructs utilizing sublaminar wires as the primary fixation, wiring alternate levels instead of every level does not compromise the stability of the construct, provided that the most proximal two levels are consecutively wired. This practice would theoretically decrease the risk of cord injury and reduce surgical time. The potential for neurologic compromise is extremely low in sublaminar wire placement. At any point during passage of the wires, if there is any resistance at all, the wire should be removed, repositioned, and then gently reinserted. Forceful insertion of sublaminar wires may result in significant inadvertent thecal sac compression. If there is excessive epidural bleeding, gentle tamponade with Gelfoam or use of bipolar electrocautery can be utilized. Expose the ligamentum flavum at the levels of anticipated wire placement. Luque double-bent wires or doubled 16- or 18-gauge wires are pre-bent at one end into a semicircular arc. To avoid inadvertent jolting and canal penetration, the sublaminar wires are usually the last bony anchors that are inserted just before performing corrective maneuvers for spinal deformities. The wires are passed in four steps: introduction, advancement, roll-through, and pull-through. The wire should be introduced at the midline of the inferior edge of the lamina. The tip of the wire should remain in contact with the undersurface of the lamina as it is advanced cranially (Fig. 28.2). The wire should be rolled so the tip emerges at the upper end of the lamina in the midline. The looped leading edge can then be grasped with a nerve hook or narrow needle holder. The wire is then pulled through by keeping a firm posterior force on the leading and trailing edge of the wire (Fig. 28.3). The wire ends are then bent to conform to the posterior lamina as described above (Fig. 28.4). At the time of rod placement, the wire ends are separated to allow the rod to rest between them. The wires are then tightened by twisting in a clockwise direction using a jet wire twister (Fig. 28.5). Retightening of the wires is often necessary before they are shortened with a wire cutter. The twisted wire ends are then twist-folded in the direction of wire twisting toward the midline posterior elements (Fig. 28.6).
Sublaminar Wire Placement
Description
Key Principles
Expectations
Indications
Contraindications
Special Considerations
Special Instructions, Position, and Anesthesia
Tips, Pearls, and Lessons Learned
Difficulties Encountered
Key Procedural Steps
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


