36 Suprapetrous Approach to Meckel’s Cave and Temporal Fossa
Daniel M. Prevedello, Amin B. Kassam, Ricardo L. Carrau, Juan C. Fernandez-Miranda, Paul A. Gardner, and Carl H. Snyderman
 Introduction
Introduction
Meckel’s cave represents a diverticulum of the dura mater within the middle cranial fossa. The periosteum layer of the dura mater maintains its dense attachment with the middle fossa bone, and the meningeal layer separates to form the space for the trigeminal nerve and Meckel’s cave. The trigeminal nerve leaves the brainstem toward the middle fossa, where it forms the gasserian ganglion and divides into three segmental branches; therefore, Meckel’s cave is also known as the trigeminal cave.1–4
Various pathologies can be encountered in Meckel’s cave. Trigeminal schwannomas and meningiomas are the most common.5–7 Other lesions include juvenile nasopharyngeal angiofibromas, chondrosarcomas, chordomas, and sinonasal malignancies, such as adenoid cystic carcinoma, which commonly spreads through the perineurium of cranial nerves.7–11
Many surgical approaches have been described to access lesions located in Meckel’s cave.1–3,12–14 These approaches can be divided in three main groups according to their anatomical route into: anterolateral, lateral, and posterolateral. None of these approaches is ideally suited to reach the entire Meckel’s cave.15 The expanded endonasal approach to the middle fossa is an alternative surgical approach that offers direct access without brain retraction.15
 Indications and Advantages
Indications and Advantages
The expanded endoscopic endonasal approach provides a direct route to the anteromedial region of Meckel’s cave. Its primary advantage is that it facilitates the dissection between the trigeminal nerve and the periosteal layer of the dura mater for lesions within the inferomedial component of Meckel’s cave. Lesions located lateral to the gasserian ganglion can also be accessed through the endonasal route using the anteromedial (V1-V2) and anterolateral (V2-V3) triangles of the middle fossa (cavernous sinus). Posterior fossa extensions can be resected in selected cases.15
The main advantage of the endonasal route is the possibility of resecting large temporal fossa/Meckel’s cave lesions without temporal lobe brain retraction.
 Contraindications
Contraindications
Complex lesions with involvement of multiple fossas or regions need to be thoroughly evaluated. If the main tumoral component of the lesion is located in the posterior fossa, then a retrosigmoid-suprameatal approach may be more appropriate. The same is valid for lesions that occupy the lateral aspect of the middle cranial or infratemporal fossa. In those cases, an open middle cranial/infratemporal approach may be more appropriate. Each patient is evaluated individually, and commonly there is a need for combining approaches to optimize the resection without transgressing the plane of cranial nerves.
 Diagnostic Workup
Diagnostic Workup
The physical examination includes a neurologic assessment, with special focus on cranial nerve function. Trigeminal sensory and motor function must be studied in detail. An ophthalmologic examination including a visual field examination is advocated for patients presenting optic nerve or orbital compromise. Endoscopic assessment of the nasal cavity is recommended to identify any nasal lesions and to document septal integrity, deviations, and other anatomical variants.
Imaging
All patients undergo a preoperative computed tomographic angiography (CTA) and magnetic resonance imaging (MRI), which are fused for intraoperative frameless stereotactic image guidance (Stryker-Leibinger Corp., Kalamazoo, MI).
 Surgery
Surgery
Instrumentation
Appropriate instrumentation is vital for the endonasal endoscopic approach to the infratemporal fossa and Meckel’s cave. Necessary equipment includes high-quality endoscopes (0-and 45-degree); videocamera and monitor; long endonasal endoscopic bipolar electrocautery; long and delicate endonasal drills with 3- and 4-mm hybrid drill tips; long dissection instruments; and hemostatic materials.
Operative Setup
Following orotracheal intubation, the patient is placed in a three-pin head holder, positioned with the head turned to the right and slightly tilted to the left.
Nasal Preparation
The nose is decongested with topical 0.05% oxymetazoline applied using ½″ × 3″ cottonoids. A povidone solution is applied to the perinasal and periumbilical areas (in case an autologous fat free graft is necessary for reconstruction).
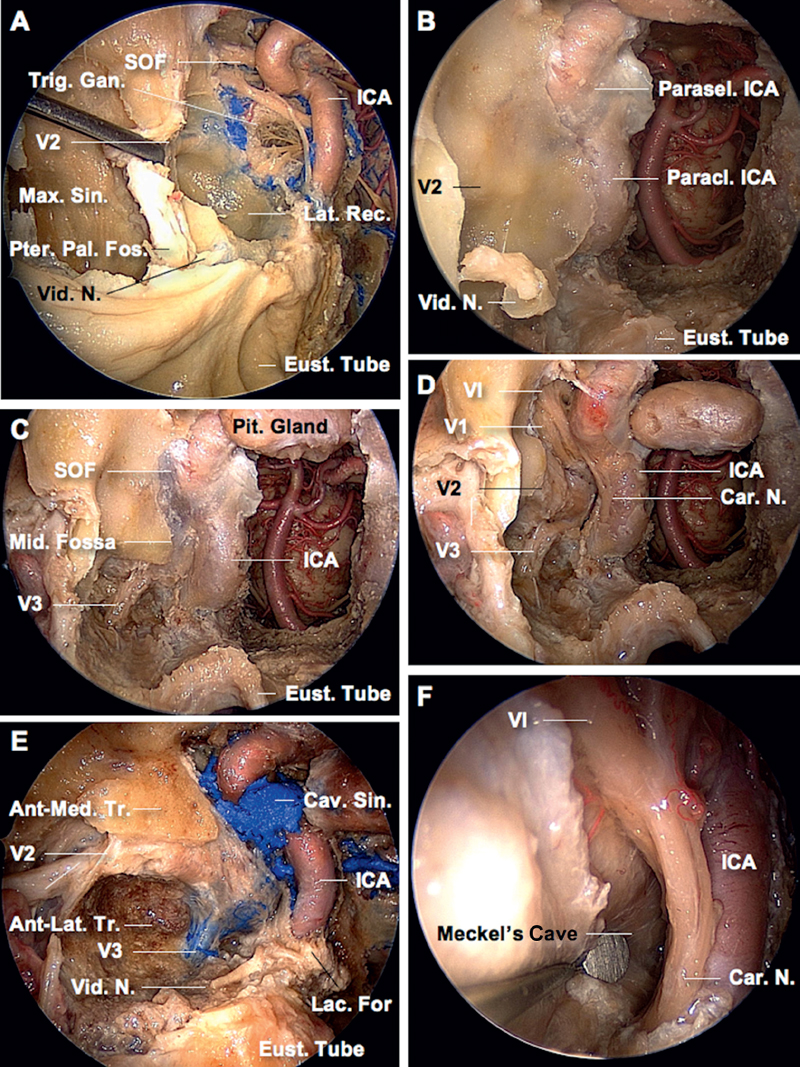
Fig. 36.1 Meckel’s cave approach. (A) A general overview of the endonasal approach to Meckel’s cave. The maxillary sinus lies anterior to the pterygopalatine fossa. Removal of the posterior wall of the maxillary sinus exposes the pterygopalatine fossa, where the vidian canal and foramen rotundum can be identified. The pterygoid process has to be drilled out to access the lateral recess of the sphenoid sinus. The vidian nerve runs in the floor of the lateral recess, and the maxillary nerve (V2) courses in the lateral wall. Both nerves tend to converge as they travel posteriorly, and are used as surgical landmarks that guide the approach. The vidian nerve, which can be preserved in selected cases, is followed posteriorly until it meets the lateral aspect of the internal carotid artery at the foramen lacerum, and the maxillary nerve is followed posteriorly where it joins the trigeminal ganglion, located posterolateral to the paraclival segment of the internal carotid artery. The superior orbital fissure, which is the anterior continuation of the cavernous sinus, is located anterosuperior to Meckel’s cave and anterolateral to the parasellar segment of the internal carotid artery. (B-F) Stepwise approach to Meckel’s cave. (B) After identifying the vidian nerve at the pterygopalatine fossa, the vidian canal is drilled out in an anteroposterior direction toward the internal carotid artery. Drilling the inferior wall of the vidian canal, pterygoid process, and upper portion of the medial pterygoid plate exposes the upper wall of the eustachian tube, which represents another important surgical landmark. Both the vidian nerve and the eustachian tube converge at the lower (or fibrocartilaginous) portion of the foramen lacerum. Remarkably, the anterior genu of the internal carotid artery (petrous-paraclival transition) occupies the upper (or vascular) portion of the foramen lacerum. Once the carotid artery has been exposed at this level, complete exposure of the paraclival and parasellar segments of the internal carotid artery is achieved. (C) Drilling now continues lateral to the paraclival carotid artery, exposing the dura of the middle fossa. The mandibular nerve and foramen ovale are identified after drilling the floor of the middle fossa. (D) The dura of the middle fossa has been opened to expose the three branches of the trigeminal nerve. The abducens nerve runs medial to the ophthalmic nerve (V1) from the cavernous sinus to the superior orbital fissure. The carotid nerve, which is a sympathetic nerve extending upward from the superior cervical ganglion along the internal carotid artery, joins the abducens nerve at the cavernous sinus. (E) An angled scope is used to inspect the regional anatomy in a different anatomical specimen. The extradural portion of the endonasal approach to Meckel’s cave has been completed. The dura covering the V2 and V3 branches remains intact. Further drilling has been performed at the anterolateral triangle of the middle fossa (between V2 and V3), whereas the osseus covering of the anteromedial triangle has not been removed. Note the confluence of the vidian nerve and the eustachian tube at the lower portion of the foramen lacerum.(F) Close-up view of Meckel’s cave. The dura that lies over the trigeminal ganglion has been opened to expose the medial aspect of Meckel’s cave. The abducens and carotid nerves are clearly identified and should be preserved during the surgical procedure. Ant.: anterior; Car.: carotid; Cav.: cavernous; Eust.: eustachian; For.: foramen; Fos.: fossa; Gan.: ganglion; ICA: internal carotid artery; Lac.: lacerum; Lat.: lateral; Max.: maxillary; Med.: medial; Mid.: middle; N.: nerve; Pal.: palatine; Paracl.: paraclival; Parasel.: parasellar; Pit.: pituitary; Pter.: pterygoid; Sin.: sinus; SOF: superior orbital fissure; Tr.: triangle; Trig.: trigeminal; Vid.: vidian.
Related posts:
 Transmaxillary Endoscopic Approach to Contralateral Parasellar Lesions
Transmaxillary Endoscopic Approach to Contralateral Parasellar Lesions



