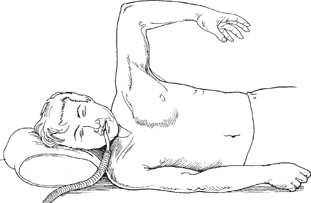
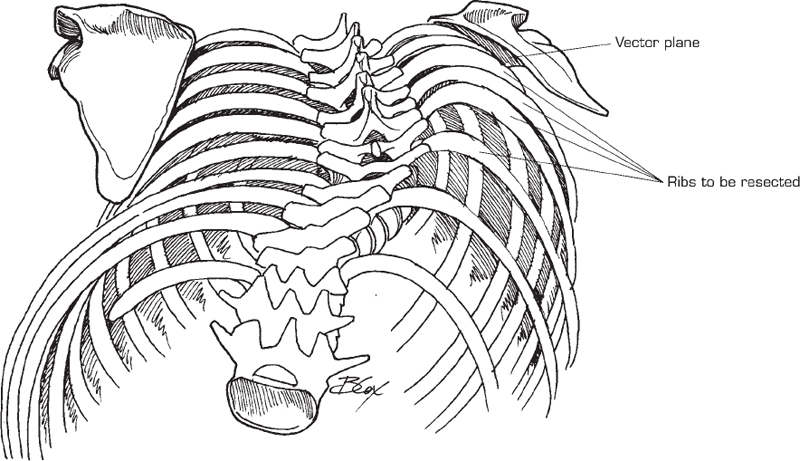
56 Carrie A. Diulus and Isador H. Lieberman Thoracoplasty is a technique involving rib resection to alleviate the cosmetic rib deformity associated with scoliosis. Cosmetic improvement of truncal appearance. Rib deformity is commonly encountered with advanced curves in patients with adolescent idiopathic scoliosis or congenital scoliosis with or without a previous posterior fusion. It may be a sequela of crankshafting after a previous posterior fusion. Patients typically present with cosmetic concerns and coronal sitting imbalance. Indications include the following: To prevent reoccurrence, delay thoracoplasty until the patient is physiologically mature. There are three techniques to perform a rib resection thoracoplasty: (1) open internal transthoracic, (2) open posterior single or double incision, and (3) endoscopic internal transthoracic. Each has its merits, and the technique used depends on the clinical circumstances. Each case should be judged on its individual merits and ultimate expectations. Fig. 56.1 Operative positioning.
Thoracoplasty: Anterior, Posterior
Description
Expectations
Indications
Contraindications
Special Considerations
Special Instructions, Position, and Anesthesia
Open Anterior Transthoracic Internal
Open Posterior with Single Midline, or Midline and Posterior Axillary Line Incisions
Endoscopic Transthoracic Internal
Tips, Pearls, and Lessons Learned
Difficulties Encountered
Related posts:
 Anterior Thoracic and Thoracolumbar Plating Techniques
Anterior Thoracic and Thoracolumbar Plating Techniques
 Anterior Cervical Corpectomy
Anterior Cervical Corpectomy
 Posterior Spinal Anchor Strategy Placement and Rod Reduction Techniques: Posterior (Rotation vs. In-Situ Translation)
Posterior Spinal Anchor Strategy Placement and Rod Reduction Techniques: Posterior (Rotation vs. In-Situ Translation)
 Iliosacral Screw Fixation Techniques
Iliosacral Screw Fixation Techniques
 Open Lumbar Microscopic Diskectomy
Open Lumbar Microscopic Diskectomy
 Spondylolysis Repair (Pars Interarticularis Repair)
Spondylolysis Repair (Pars Interarticularis Repair)
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


