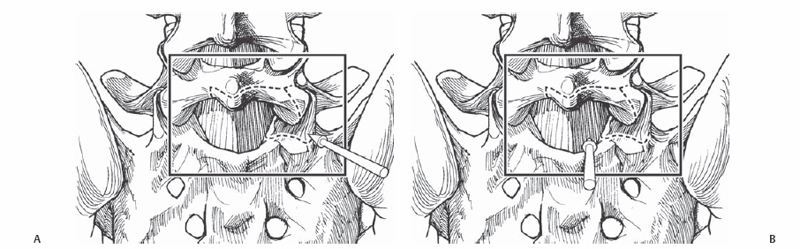
38 Todd J. Albert and Peter M. Fleischut The goal of transforaminal lumbar interfusion (TLIF) is to safely access the interbody area without significant dural retraction. This allows one to effectively fuse both anteriorly and posteriorly through a posterior only approach. Posterior lumbar interbody fusion (PLIF) achieves similar goals through a bilateral, more medial approach. PLIF requires more dural retraction than TLIF, which is essentially a far lateral PLIF. Anterior interbody support facilitates deformity correction, increased fusion rate, and disk space distraction, as well as at least unilateral if not bilateral direct foraminal decompression and traversing nerve root decompression. An improved fusion rate compared with a posterior lateral intertransverse process fusion. A PLIF or TLIF at the end of a long fusion decreases the risk pseudarthrosis due to improved anterior column support. Isthmic spondylolisthesis (grades 1 to 4), junctional degeneration adjacent to a fusion mass, degenerative disk disease, recurrent disk herniation with significant back pain, the terminal end of long fusion requiring interbody fusion, short segment degenerative scoliosis, postlaminectomy spondylolisthesis. Severe osteopenia, bleeding disorders, and active infection. Preoperative imaging studies including anterior/posterior and flexion/extension lumbosacral spine radiographs are necessary. Additionally, magnetic resonance imaging (MRI) or computed tomography (CT) myelography is necessary for understanding the anatomy and planning the surgical approach (left versus right or unilateral exposures). At times for discogenic back pain, diskography, though controversial, can be useful in determining the level of the pain generator. The patient should be placed prone with the abdomen decompressed. An Andrews frame is generally used for L4-sacrum exposures. For longer approaches such as adult deformity, a Jackson table is used. Triggered electromyography (EMG) recording can be used to test the accuracy of pedicle screw placement. Free-run EMG recording can be used during insertion of transforaminal lumbar interbody fusion grafts or cages to ensure that undue traction or injury is avoided to the exiting or traversing nerve roots. Complete radical diskectomy requires use of multiple interbody instruments including angled curettes and osteotomes (straight and angled and double-angled chondrotomes to scrape the end plates and remove the maximum amount of disk material from one side to the other if a unilateral approach is used [TLIF]). Special intervertebral distraction devices are helpful. In the TLIF procedure, the inferior articular process of the vertebra above is taken off to gain access to the transforaminal area and the superior articular process of the vertebra below is skeletonized to maximize the transforaminal opening. Bullet distractors are an optimal distraction instrument to obtain maximum annulotaxis. A large lamina spreader placed between the spinous processes also assists in disk space distraction, though this method risks a kyphosing force on the disk space. This technique of overdistraction is helpful when placing a banana-shaped cage through a unilateral TLIF approach and is often not necessary in a bilateral PLIF cage approach. For interbody grafting, various approaches can be applied. Carbon fiber, metallic, or poly-ether-ether-ketone (PEEK) type cages in rectangular, bulleted, or banana shapes can be used. Maximum lordosization is achieved by placing the cage, especially a banana-shaped cage, in the anterior part of the disk space. Finally, with the anterior interbody device anteriorly situated, a compressive force is placed across the pedicle screw instrumentation to enhance lordotic alignment. Hemostasis is obtained by using bipolar cautery in the area just medial to the pedicle and in the axilla of the exiting nerve root where the majority of work is to be done. Significant bleeding can occur during these procedures, and there may at times be difficulty with interspace distraction. In cases with excessive bleeding, or with difficulty with interspace distraction, a non-structural graft may be used.
Transforaminal and Posterior Lumbar Interbody Fusion
Description
Key Principles
Expectations
Indications
Contraindications
Special Considerations
Special Instructions, Position, and Anesthesia
Tips, Pearls, and Lessons Learned
Difficulties Encountered
Key Procedural Steps
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


