Chapter 14 Visual Loss
Visual loss commonly accompanies neurological disease and is one of the most disturbing symptoms a patient may experience. While visual loss is often due to a benign or treatable process, it can be the first sign of a blinding or life-threatening disease. Common causes of visual loss include uncorrected refractive error, corneal disease, cataract, glaucoma, retinal and choroidal disease, and amblyopia. Ophthalmic causes of visual loss are often not apparent to the neurologist, whereas neurological causes of visual loss often confuse ophthalmologists. Thus, the approach to evaluating visual loss must be systematic, so that important causes are not missed and simple causes are not overinvestigated. In this chapter, we discuss the patterns and temporal profiles of visual loss; examination techniques are discussed in Chapter 36 and funduscopic abnormalities are discussed in Chapter 15.
Pattern of Visual Loss
Central Visual Loss
A defect in the visual field surrounded by normal vision is called a scotoma, from the Greek word meaning “darkness.” Loss of central vision, resulting in a central or cecocentral scotoma, is usually quickly noticed and reported. Peripheral visual field defects, such as homonymous hemianopia, can be asymptomatic but when noticed are frequently referred to the eye with the greater extent of field loss (i.e., the eye with temporal field loss) (Fig. 14.1). Central and cecocentral scotomas are usually due to lesions of the central retina or optic nerve. When the lesion is at the junction of the optic nerve and chiasm, there will be an ipsilateral central scotoma due to optic nerve involvement, and a contralateral temporal defect due to chiasmal involvement; this highly-localizing visual field defect is known as a junctional scotoma (Fig. 14.2). Patients with junctional scotomas are often unaware of the contralateral temporal defect, emphasizing the importance of assessing each eye separately during history taking and visual field evaluation.
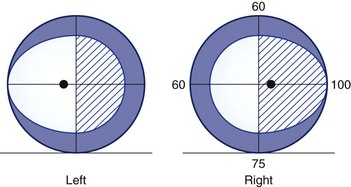
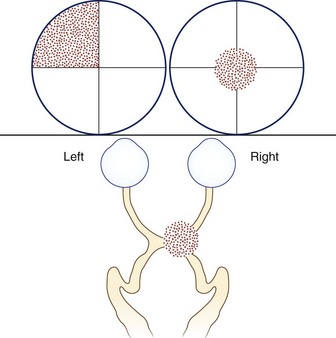
Fig. 14.2 Junctional scotoma from a lesion at the junction of the optic nerve and chiasm. The lesion affects both the right optic nerve, producing a cecocentral scotoma in the right eye, and crossing fibers in the optic chiasm, producing an upper temporal visual field defect in the left eye. The temporal field defect of a junctional scotoma often goes unnoticed by the patient and may only be detected with visual field testing (see Chapter 36).
In general, scotomas caused by retinal disease are so-called positive scotomas, since they are perceived as a black or gray spot in the visual field. Patients with macular pathology can also have metamorphopsia, where there is distortion of images such that straight edges or geometrical figures appear warped. Metamorphopsia is almost always caused by retinal disease. In contrast, optic nerve lesions characteristically produce negative scotomas, areas of absent vision that are otherwise not perceivable, in conjunction with decreased color vision, contrast vision, and light brightness perception. On occasion, paradoxical photophobia, especially with fluorescent lighting, can occur with optic nerve lesions. Photopsias (light flashes) can occur with vitreoretinal traction (e.g., posterior vitreous detachment), retinal disease (e.g., cancer-associated retinopathy), toxicity from certain drugs (e.g., digitalis), or optic nerve disease (e.g., in the healing phase of optic neuritis, in which case they may be evoked by sound). Photopsias can also occur as part of migrainous visual aura. Aside from ocular diseases, bilateral central visual loss can result from lesions involving both optic nerves, the optic chiasm, or the part of the occipital cortex concerned with central vision. The possibility of nonorganic visual loss must also be considered, but it remains a diagnosis of exclusion (see Chapter 36).
Peripheral Visual Loss
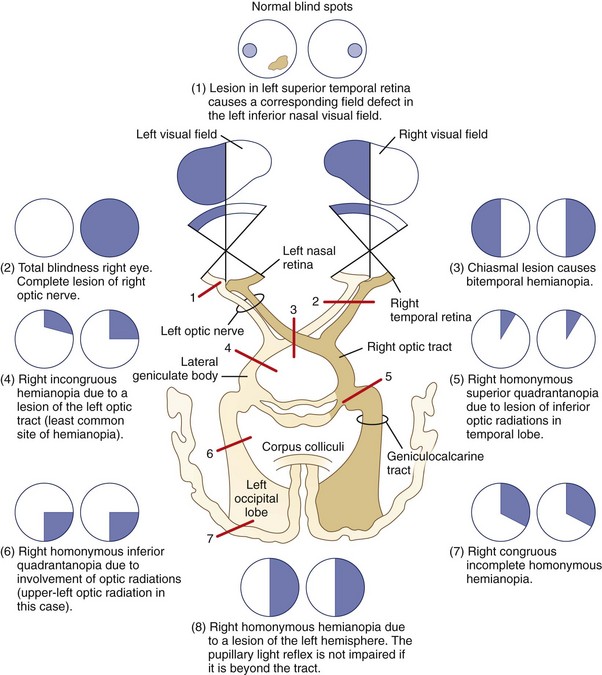
For simplicity, visual field defects can be classified into one of three groups: prechiasmal, chiasmal, or retrochiasmal. Unilateral prechiasmal lesions affect the visual field of one eye only, chiasmal lesions affect the fields of both eyes in a non-homonymous bitemporal fashion, and retrochiasmal lesions cause homonymous field defects with variable degrees of congruity (i.e., similarity) depending on their location (Fig. 14.3). See Chapter 36 for further discussion of patterns of visual field loss.
Temporal Profile of Visual Loss
Sudden-Onset Visual Loss
Visual loss of sudden onset can be divided into three temporal patterns: transient (Box 14.1) (Thurtell and Rucker, 2009), nonprogressive, and progressive.
Box 14.1 Causes of Transient Monocular Visual Loss
Transient Monocular Visual Loss
Amaurosis Fugax
The term amaurosis fugax is often used to describe the transient monocular visual loss (TMVL) caused by emboli from the carotids, aortic arch, or heart to the retinal circulation. Typically, these attacks are sudden in onset, last from several to 15 minutes, and are characterized by altitudinal visual field loss that is often described as being like a curtain descending over the eye (Donders, 2001). Patients may also describe having separate attacks with hemispheric symptoms, such as weakness and speech disturbance, rather than visual loss.
Retinal Artery Vasospasm
Transient monocular visual loss can be caused by retinal artery vasospasm and is called retinal migraine when accompanied by migraine headache (Hill et al., 2007). Vasospastic TMVL is usually benign and often responds to calcium channel blockers (Winterkorn et al., 1993).
Visual Loss in Bright Light
Some patients with reduced blood supply to the eye due to a high-grade stenosis or occlusion of the internal carotid artery report TMVL in bright light, which is likely due to impaired regeneration of photopigments secondary to ocular ischemia (Kaiboriboon et al., 2001). The TMVL can also occur following meals or with postural changes. A variety of ophthalmic abnormalities, including midperipheral retinal hemorrhages, can be present and collectively comprise the ocular ischemic syndrome (Chen and Miller, 2007). Other retinal diseases, such as cone dystrophies and age-related macular degeneration, can cause evanescent visual loss in bright light, also known as hemeralopia or day blindness. The visual loss in these diseases is usually bilateral, whereas it is unilateral in patients with unilateral carotid disease.
< div class='tao-gold-member'>






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


